- Visibility 58 Views
- Downloads 6 Downloads
- DOI 10.18231/j.ijpo.2022.008
-
CrossMark

Study of cyto-histopathological correlation in thyroid lesions at rural tertiary care hospital
- Author Details:
-
 Mangala Rajesh Nagare
Mangala Rajesh Nagare
-
Sneha R Joshi *
Introduction
Thyroid lesions are common among all endocrine disorders. In clinical practice, a majority are benign but in a significant percentage them are underlying malignant.[1], [2] It is difficult to overall diagnose based only on clinical evaluation. Therefore, it is essential that a correct diagnosis is made as early as possible.[3]
As we know, thyroid lesions are very common in surgical practice and their worldwide prevalence is 4-7%. The incidence of malignancy in thyroid goiter is 10%. It affects women more commonly than men. It is not practical to excise all the thyroid lesions because of certain risks associated with it. To avoid unwanted surgery, an effective screening test is required.[4]
In the management of thyroid lesions, fine needle aspiration cytology (FNAC) has been accepted as the first-line investigation, especially for solitary nodules. It is a screening tool to decide whether a patient needs surgical intervention or can be managed conservatively.[5] Fine needle aspiration cytology (FNAC) is simple, cheap, easily available, reliable, time saving, easy to perform, effective and almost accurate diagnostic technique for investigation of thyroid swelling.[6], [7], [8]
FNAC has its limitations like sample adequacy, techniques of sampling, experience of the cytopathologists. Also, there are difficulties in differentiating between benign and malignant follicular neoplasms because of many overlapping cytological features. Hence for final diagnosis,” histopathological examination” is necessary.[9], [10]
Materials and Methods
This observational Prospective study was conducted in the Department of pathology of our hospital, MIMER Medical College Talegaon (D), Pune, India, between Oct 2015 to August 2016 in collaboration with Department of Surgery and Radiology.
Inclusion criteria
All the patients coming our hospital with thyroid lesions irrespective of age and sex was included in present study.
Sample collection and method
All the patients were clinically examined in detail according to the proforma and a careful palpation of the thyroid was done to guide precisely the location for doing aspiration. Details of the procedure were explained to the patients. Aspiration was done with the patient lying comfortably in a supine position and the neck was extended with a pillow under the shoulder so as to make the thyroid swelling appear prominent.
FNAC was performed under all aseptic precaution, with help of 23 gauge needle and disposable 5ml/10ml syringes. Whenever needed USG guided FNAC was done. Smears was prepared, fixed in 95% ethyl alcohol and Stained with hematoxylin & eosin stains FNAC smears were carefully studied and categorized into non neoplastic and neoplastic lesions.
Ethical clearance
Clearance from the Institutional Ethical committee was obtained.
(Ethical Approval letter no. : 222. Date-16-10-2014.)
Statistical analysis
Statistical analysis was done with appropriate tests in consultation with a statistician.
Results
The present study deals with the fine needle aspiration cytology of thyroid lesions and determination of diagnostic accuracy of aspiration cytology. A total of 111 patients with thyroid lesions were subjected to fine needle aspiration cytology during a period of 2 years. Of these 65 patients underwent surgery subsequently and the excised specimens were sent to the Department of Pathology for histopathological examination. Correlation between FNAC and histopathological study was done.
Sex distribution
Majority of the patients referred for FNAC thyroid were females constituting 87 (78.32%) of the total 111 patients, and 24 male cases (21.81%). Male to female ratio was 1:3.58.
Age distribution
Age of the patients ranged from 10 years to75 years with a median age of 39 years. The maximum incidence of thyroid lesions was noted in the 31 to 40 years age group in which there were 33 cases (29.72%). This was followed by the 21 to 30 years of age group and 41 to 50 years of age group with an incidence of 27.02% (30 cases) and 24.32% (27 cases).
Fine needle aspiration cytology
In the present study, non-neoplastic lesions were more commonly encountered than the neoplastic lesions, cytological evaluation of the lesions was performed based on standard criteria reported in the literature.
Cytologic diagnosis was classified as
Non-neoplastic category
Smears with large quantity of colloid and several groups (generally six or more) of normal appearing follicular cells with or without the presence of histiocytes. The benign lesions include colloid nodule, nodule goiter, thyroiditis and thyroid cysts.
Neoplastic category
It includes both benign and malignant neoplasms. The aspirations which contained groups of cells with malignant features were considered diagnostic of primary thyroid cancer (papillary, medullary or anaplastic subtypes) or disease metastatic to thyroid. Histopathologic evaluation was advised because the criteria of malignancy in these lesions are based on evidence of capsular or vascular invasion.
Insufficient/inadequate category
Smears showing a minimum of six clusters of well-preserved follicular cells with each group containing at least 10 cells were considered adequate. Aspirates considered in sufficient had only blood or cyst fluid or scattered thyroid cells fewer than above mentioned number without colloid.
Total number of cytological diagnosis was 111. Amongst them 91.89% were non-neoplastic and 7.20% were neoplastic. ([Table 1])
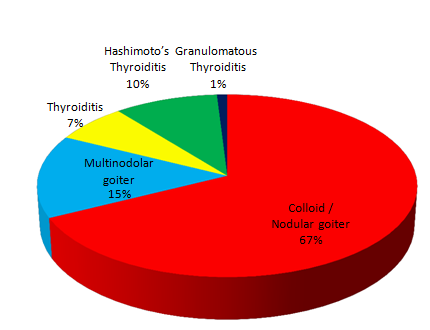
In the present study among 111 patients, nodular / colloid goiter were most common lesions accounting for 69 cases (67.64%) followed by Multinodolar goiter which were 15 cases (14.70%). ([Figure 1])
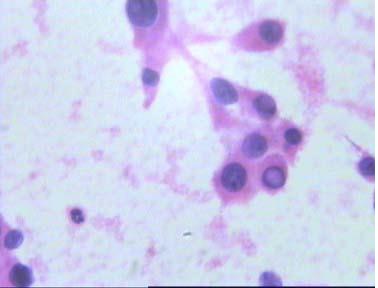
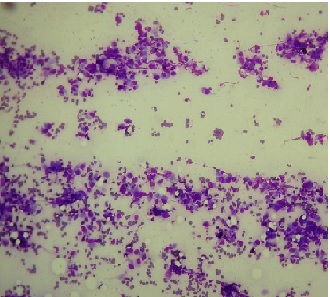
In the present study, of total 8 neoplastic cases, majority of the cases were of suspicious for follicular neoplasm (4 cases) ([Figure 3]). This was followed by suspicious for papillary carcinoma (2 cases) ([Figure 4]), medullary carcinoma (1 case) and undifferentiated (Anaplastic) carcinoma(1 case) ([Figure 5]). In present study cytological diagnosis of suspicious of follicular neoplasm was made in 4 cases out of 111.


|
Cytological diagnosis- |
Number(n) |
Percentages (%) |
|
Non-Neoplastic |
102 |
91.89 |
|
Neoplastic |
08 |
7.20 |
|
Inadequate |
01 |
0.90 |
|
Total |
111 |
100 |
|
Histopathological Diagnosis |
Number |
Percent (%) |
|
Follicular adenoma |
3 |
30 |
|
Follicular carcinoma |
2 |
20 |
|
Papillary carcinoma |
2 |
20 |
|
Medullary carcinoma |
1 |
10 |
|
Undifferentiated (anaplastic) thyroid carcinoma |
2 |
20 |
|
Total |
10 |
100 |
|
Histological diagnosis |
No. of patients |
Cytological Diagnosis |
|||
|
Correlated |
Non-Correlated |
||||
|
No. of patients |
Percentage (%) |
No. of patients |
Percentage (%) |
||
|
Non-Neoplastic lesions |
55 |
54 |
98.18 |
01 |
1.81 |
|
Follicular neoplasms |
05 |
04 |
100 |
- |
- |
|
Medullary carcinoma |
01 |
01 |
100 |
- |
- |
|
Papillary carcinoma |
02 |
02 |
100 |
- |
- |
|
Anaplastic carcinoma |
02 |
01 |
50 |
01 |
50 |
|
Total |
65 |
63 |
96.92 |
02 |
3.07 |
|
Author |
Hyang-MiKo et al [11] |
Gupta et al [8] |
Bashrat et al [12] |
Pandey et al [9] |
Chetna Sharma [13] |
Present Study |
|
Year |
2003 |
2010 |
2011 |
2012 |
2015 |
2016 |
|
No.of cases |
207 |
75 |
50 |
447 |
945 |
111 |
|
Sensitivity (%) |
78.4 |
80 |
80 |
57.14 |
89.5 |
88 |
|
Specificity (%) |
98.2 |
86.6 |
97.70 |
90 |
98 |
100 |
|
PPV (%) |
99 |
80 |
80 |
70.58 |
84.6 |
100 |
|
NPV (%) |
66.3 |
86.6 |
97.70 |
83.33 |
98.6 |
98.21 |
|
Accuracy (%) |
84.4 |
84 |
96 |
80.28 |
97 |
95.45 |
The cytological diagnosis of suspicious for papillary carcinoma was given in two cases. There was one case of medullary carcinoma and one case of anaplastic carcinoma on cytology. ([Figure 2])
In the present study following neoplastic lesions of thyroid were found - follicular adenoma, follicular carcinoma, papillary carcinoma, medullary carcinoma, undifferentiated (anaplastic) thyroid carcinoma ([Table 2])
In present study the cytology - histopathology concordance rate for Non-neoplastic lesions and neoplastic lesions was as follows –
Non-neoplastic lesions-98.18%
Neoplastic lesions – 90%
Discussion
For preoperative investication of thyroid nodules, fine needle aspiration cytology is a well-established technique. To differentiate between benign and malignant thyroid nodules, this non-invasive technique is an efficient method.[12], [14], [15]
According to several investigators, the fine needle aspiration cytology is a useful tool for selecting patients with nodular thyroid disease for thyroidectomy.[12], [15], [16]
In the present study, age of the patients ranged from 10-75 years with a median age of 39 years.
This was comparable to Rabia Basharat et al, [12] Pandey et al,[9] Herachand et al,[15] Rangaswamy et al.[17]
The number of males in the present study was 24(21.62%) and females were 87 (78.37%) with a male to female ratio of 1: 3.62. Sex distribution was comparable with Rangaswamy et al,[17] Afroze N et al.[18]
In the present study, the most common lesion was Nodular/colloid goiter accounting for 69 (67.64%) followed by thyroiditis, 18 cases (16.21%) and Multinodular goiter, 15 cases (14.70%). A comparable observation was made by Handa et al. where 250 cases (65.6%) were colloid goiter and thyroiditis were 119 cases (31.23%).
The next common was follicular neoplasm (4 cases), papillary carcinoma (2 cases, anaplastic carcinoma (2 cases) and medullary carcinoma (1 case). Distribution was comparable with Handa et al,[19] Richard et al[16] and Bagga & Mahajan et al.[3]
In the present study of total 111 cases diagnosed on cytology, surgical sample were available for 65 cases, of this 62 cases correlated with histopathological findings, 1 case which was reported as inadequate on cytology was diagnosed as microfollicular adenoma on histopathology. This was because of presence of very tiny lesion that was missed during aspiration.
In the present study the false negative rate is 1.5%. This figure is in agreement with the other studies which reported false negative rate between 1- 11%. 64 false negative rate is a concern because a missed malignant lesion will result in direct consequences for the patient.
In the present study 2 cases were diagnosed as papillary carcinoma on cytology which proved to be papillary carcinoma on histopathology. Hyang Mi Ko et al,[11] has reported the predictive value of a cytologic diagnosis as 100% for papillary carcinoma. In present study no false positive case (0%) was diagnosed. This is in agreement with other studies which reported false positive error rates between (0-9%)
In the present study majority of the lesions were non-neoplastic 84.61% (55 cases) and 10 were neoplastic (15.38%) cases percentage was similar to Safirullah et al[20] and Kamal et al.[21]
Statistical analysis of Malignant lesions showed accuracy, sensitivity, specificity, positive predictive value and negative predictive value of FNAC to be 95.45%, 88%, 100%, and 100%, 98.21% respectively. These results are comparable to the study done by Afroze et al[18] where malignancy showed 1) sensitivity of 61.90%, 2) specificity of 99.31%, 3) positive predictive value of 92.86%, 4) Negative predictive value of 94.74%, 5) Accuracy of 94.58%. ([Table 4])
Conclusion
Fine needle aspiration cytology of thyroid is simple diagnostic tool with sensitivity 88% and specificity 100%. It has certain limitations but it gives guidelines to clinicians about further management of various thyroid lesions.
Source of Funding
None.
Conflict of Interest
No conflict of interest.
References
- GH Sakorafas. Thyroid nodules; interpretation and importance of fine-needle aspiration (FNA) for the clinician - practical considerations. Surg Oncol 2010. [Google Scholar]
- TT Htwe, MM Hamdi, GK Swethadri, JO Wong, MM Soe, MS Abdullah. Incidence of thyroid malignancy among goitrous thyroid lesions from the Sarawak General Hospital. Singapore Med J 2000. [Google Scholar]
- PK Bagga, NC Mahajan. Fine needle aspiration cytology of thyroid swellings: how useful and accurate is it?. Indian J Cancer 2010. [Google Scholar]
- SS Mangshetty, R Jewargikar, SK Andola. Fine Needle Aspiration Cytology of 220 Thyroid Lesions Histopathological Correlation. Int J Res Health Sci 2014. [Google Scholar]
- N Mamoon, R Jamy, AH Khan. Evaluation of fine needle aspiration cytology as a screening tool in thyroid lesions. J Pak Med Assoc 2013. [Google Scholar]
- LG Koss. . Diagnostic cytology and its histopathologic basis 1992. [Google Scholar]
- R Nepali, V Banita, G Takur. Comparative study of FNAC and histopathology in the diagnosis of thyroid swelling. Internet J Head Neck Surg . [Google Scholar]
- M Gupta, S Gupta, V Gupta. Correlation of fine needle aspiration cytology with histopathology in the Diagnosis of Solitary Thyroid Nodule. J Thyroid Res 2010. [Google Scholar]
- P Pandey, A Dixit, NC Mahajan. Fine-needle aspiration of the thyroid: A cytohistologic correlation with critical evaluation of discordant cases. Thyroid Res Pract 2012. [Google Scholar]
- S Chandanwale, N Singh, H Kumar, P Pradhan, C Gore, M Rajpal. Clinicopatholological correlation of thyroid nodules. Int J Pharm Biomed Sci 2012. [Google Scholar]
- R Basharat, MH Bukhari, S Saeed, T Hamid. Comparison of fine needle aspiration cytology and thyroid scan in solitary thyroid nodule. Patholog Res Int 2011. [Google Scholar]
- HM Ko, IK Jhu,, SH Yang, JH Lee, JH Nam, SW Juhng. Clinicopathologic analysis of fine needle aspiration cytology of the thyroid. A review of 1,613 cases and correlation with histopathologic diagnoses. Acta Cytol 2003. [Google Scholar]
- C Sharma. Diagnostic accuracy of fine needle aspiration cytology of thyroid and evauation of discordant cases. J Egypt Natl Canc Inst 2015. [Google Scholar]
- JF Nasuti, PK Gupta, ZW Baloch. Diagnostic value and cost-effectiveness of on- site evaluation of fine- needle aspiration specimens: review of 5,688 cases. Diagn Cytopathol 2002. [Google Scholar]
- M Hirachand, M Lakhey, R Thapa, S Kafle. Accuracy of fine needle aspiration cytology in diagnosis of thyroid swelling. J Pathol Nepal 2013. [Google Scholar]
- RA Prinz, PJ O'Morchoe, AL Barbato, SS Braithwaite, MH Brooks, MA Emanuele. Fine Needle Aspiration Biopsy of Thyroid Nodules. Ann Surg 1983. [Google Scholar]
- M Rangaswamy, K Narendra, S Patel, C Gururajprasad, V Manjunath. Insight to neoplastic thyroid lesions by fine needle aspiration cytology. J Cytol 2013. [Google Scholar]
- N Afroze, N Kayani, SH Hasan. Role of fine needle aspiration cytology in the diagnosis of palpable thyroid lesions. Indian J Pathol Microbiol 2002. [Google Scholar]
- U Handa, S Garg, H Mohan, N Nagarkar. Role of fine needle aspiration cytology in diagnosis and management of thyroid lesions: A study on 434 patients. J Cytol 2008. [Google Scholar]
- MN Safirullah, A Khan. Role of fine needle aspiration cytology (FNAC) in the diagnosis of thyroid swelling. JPMI 2004. [Google Scholar]
- MM Kamal, DG Arjune, HR Kulkarni. Comparative study of fine needle aspiration and fine needle capillary sampling of thyroids lesions. Acta Cytol 2002. [Google Scholar]