Introduction
Fungi are ubiquitous organisms among which almost 300 species are found to be pathogenic to humans. The manifestations can be as superficial or deep seated infections. Invasive or disseminated fungal infections are rare and occur mainly in the setting of immunocompromised state. Disseminated fungal infection is the presence of a fungal pathogen in the blood (fungemia) and/or any other deep-seated site because of hematogenous seeding. Conditions which predispose individuals for disseminated fungal infections include renal failure, following surgical procedures, HIV, neutropenia, hematological malignancies, long term use of antibiotics, late sepsis and total parenteral nutrition.
Candida is the commonest pathogen encountered in disseminated fungal infections. Secondary seeding of the organism can occur as a result of hematogenous spread and involves almost every organ including brain, heart, kidneys, liver, bones, muscles, joints, spleen and eyes. Candida albicans is a normal commensal in the mouth, throat, vagin skin and human gastrointestinal tract. The vast majority of cases of invasive candidiasis is caused by Candida albicans. When perturbations of mucosal microbiota or weakening of host immune response occur, Candida species undergo transition from commensalism to opportunism. Cell-mediated immunity plays a major role in protection against candidiasis. So any disease states with hampered cell mediated immunity, as in HIV, will predispose individuals to invasive candidiasis. Mortality from disseminated fungal disease is high and therefore high index of suspicion, prompt diagnosis and prompt initiation of antifungal therapy is essential.1, 2, 3, 4, 5
Here we report a case of disseminated candidiasis which masqueraded as adrenocortical carcinoma an adult male who was found to be HIV positive on pre operative evaluation.
Case Report
45 year old male presented to the surgical OPD with complaints of loss of appetite, abdominal pain, dizziness and weakness of lower limb for 2 months. Blood investigations revealed anemia (Hb-7.8g/dl), leucopenia (total count-3500/c.mm) and elevated ESR (150mm/hr.). Serological examination showed HIV positive ELISA.CT abdomen was done and showed right sided adrenal mass and was suggestive of adrenocortical carcinoma/metastasis. AFB smear was negative.
Excision of the right adrenal mass was done and sent for histopathological examination. Part of the tissue and the pus collected intraoperaively was also sent for microbiological culture studies. The clinical differential diagnoses were adrenocortical carcinoma & tuberculosis.
Grossly we received a fibrofatty soft tissue fragment measuring 8x7x3cm with cut section showing grey white to tan brown areas with cystic spaces showing pus like material. (Figure 1)
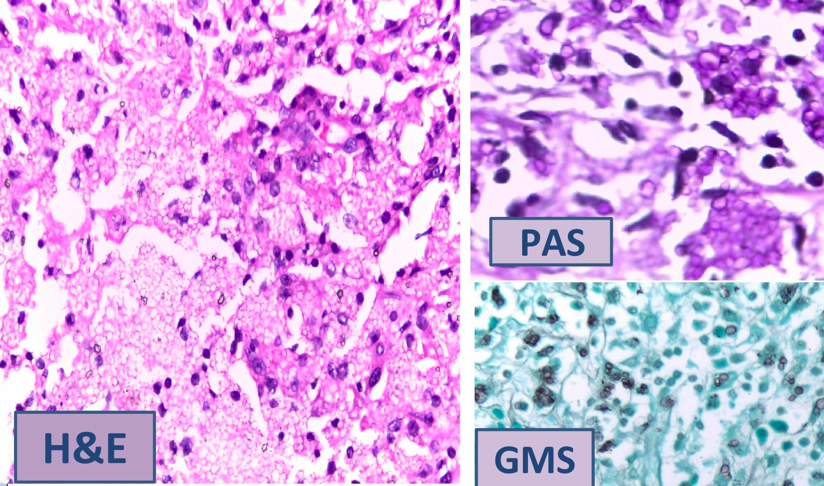
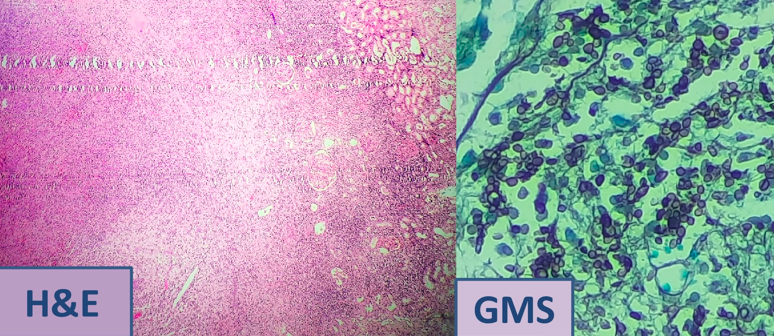
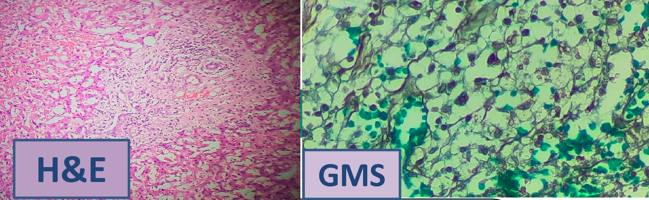
Microscopic examination revealed adrenal gland with extensive areas of necrosis and a dense inflammatory infiltrate of lymphocytes,neutrophils,eosinophils and plasma cells along with numerous foamy histiocytes showing intracellular and extracellular round bodies(budding yeast forms). Liver tissue and a segment of renal cortical tissue was also identified in the sections which also showed similar organisms. Special stains for fungi (PAS & GMS) were positive and revealed the numerous budding yeast forms and very few hyphael forms.
Thus, a histopathological diagnosis of a chronic suppurative inflammatory lesion with intracellular and extracellular yeast like fungi suggestive of disseminated deep fungal infection involving adrenals, liver and kidney was given. The possibilities of blastomycosis, Candiasis and histoplasmosis were included in the differential diagnosis. Microbiological culture studies was advised mandatory to confirm the diagnosis and for species identification. (Figure 2, Figure 3, Figure 4)
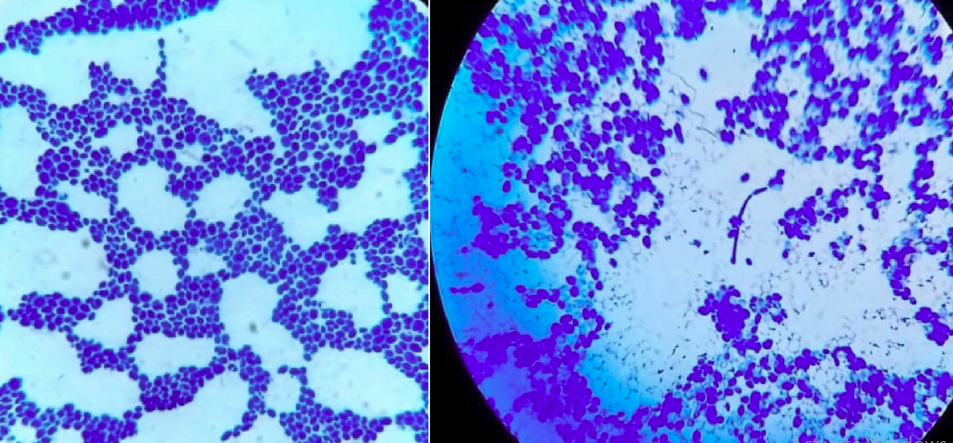
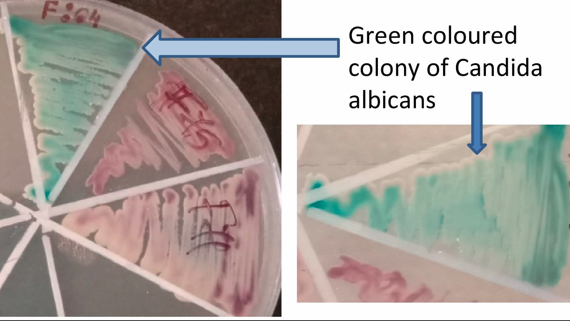
Gram stain revealed numerous budding yeast forms of candida and microbiological culture studies revealed green coloured colonies in chrome agar plate suggestive of Candida albicans.(Figure 5, Figure 6)
Thus, the diagnosis of disseminated candidiasis, species being candida albicans was confirmed.
The patient was started on anti-retroviral drugs along with systemic antifungals and other supportive medications and is currently doing well.
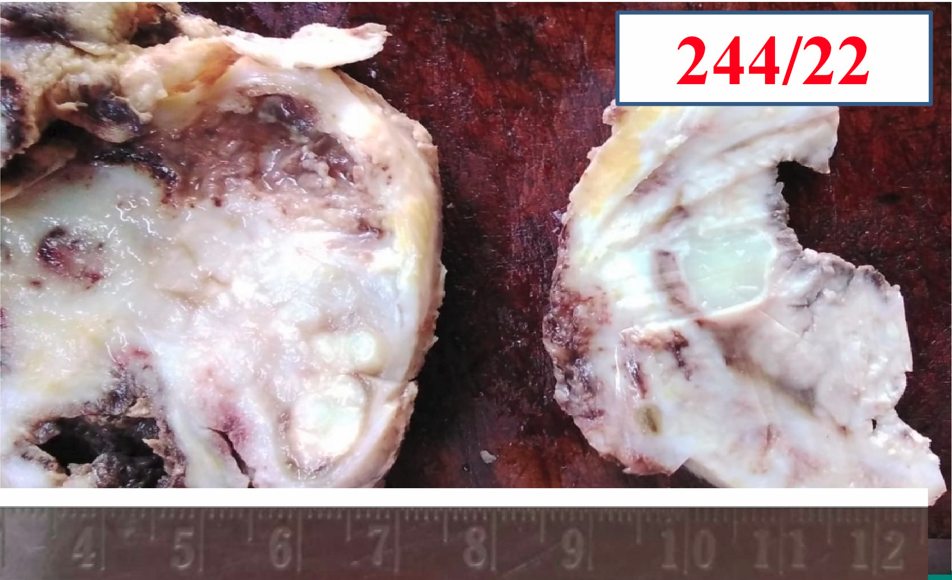
Figure 2
H&E sections from adrenal gland showing budding yeast forms; special stains for fungi-PAS & GMS
Discussion
Candidiasis is an infection caused by a yeast type of fungus called Candida. Candida species can cause localized superficial infections in the mouth and throat (also called “thrush”) or in the vagina which can be easily treated with local antifungal applications or oral antifungal drugs. But invasive candidiasis is a serious infection that can affect the blood, heart, brain, eyes, bones, and other parts of the body and will require aggressive systemic therapy.
Among the pathogenic fungi Candida and aspergillus are the commonest causes of disseminated fungal infection. An increasing number of non-Candida yeasts and non-Aspergillus moulds have recently emerged as important causes of invasive disease.4 Among the different species of candida, C.albicans, C.glabrata, C.tropicalis, C.parapsilosis, C.krusei and C.auris are implicated in disseminated infections. Candida albicans causes almost 50% of cases of disseminated mycosis. Invasive candidiasis is rare among immunocompetent individuals, but can evolve into a fatal disseminated infection in immunosuppressed individuals. Cell mediated immunity is important in protecting against fungal infections. So, any deficiency in cell mediated immunity can predispose individuals to systemic and disseminated fungal infections.3
Invasive candidiasis is associated with high mortality of 40-70%, if not treated aggressively. Death mainly occurs due to sepsis despite advances in antifungal therapy.
The diagnosis needs to be confirmed by histopathological examination and species identification is to be done with microbiological culture studies. In H&E and with fungal stains like PAS and GMS candida appear as mats of budding yeast forms, measuring about 3-5 micrometers intermingled with pseudo hyphae along with a mixed inflammatory infiltrate, micro and macro abscesses. Granulomas are rare. On culturing in chrome agar, Candida albicans grow as green coloured colonies.5
Conclusion
This case is being reported to highlight the fact that invasive or disseminated fungal infections are very common in the setting of an immunocompromised state and is a major cause of morbidity and mortality. This can be prevented by prophylactic medications in patients at high risk and also by definitive treatment when diagnosis is confirmed. Key challenges to the management of invasive candidiasis include prevention, early recognition and rapid initiation of appropriate systemic antifungal therapy. A high index of suspicion, followed by prompt diagnosis and aggressive treatment is essential to prevent mortality.