Introduction
A haematological malignancy arises when something goes wrong in the regulation of the division or the life span of a blood cell or its precursor.1 It is characterized by widespread, rapid and disorderly proliferation of leukocytes and their precursor and by the presence of immature leukocytes in blood often in very large numbers. Leukemia is malignant neoplasm of hematopoietic stem cells characterised by diffuse replacement of the bone marrow and/or peripheral blood by neoplastic cells. It is one of the most frequently occurring cancers in all races or ethnicities with relative proportion vary between 25-40%.2 They are usually divided into myeloid and lymphoid, acute and chronic. This simple classification based on lineage and on rate of disease progression when untreated. The purpose of classification of leukemias is to organise knowledge into manageable forms so that biological entities can be recognised. Correct classification permits optimal patient management.3 They are the 10th most common cancer in men and 12th most common in women and constitute 3% of the global cancer burden.4 The cell type distribution of leukemias observed in India is different from that observed in developed world. Myeloid leukemias predominate in India while lymphoid leukemias dominate in western world mainly because of higher incidence of chronic lymphatic leukemia.3 Leukemia symptoms can occur all of a sudden or gradually. Fever, infection is seen as WBC count gets down. Fatigue, physical exercise intolerance, abdominal pain, or generally feeling fullness, weight loss appears due to reduction in normal erythrocytes. Bleeding is common as platelet number is less. In 2017, males have been accounted for more than 37 percent of the new cases of leukaemia. High incidence of subtypes of leukemia in males was due to more exposed to occupational and environmental carcinogen.5, 6 Age, sex have played a vital role in learning about the causes of leukemia in the past few decades. The developing countries have greater burden of cancer including haematological malignancies due to population growth, aging and urbanization, changing dietary habits, better control of infections, and increasing tobacco consumption.7 This is further challenging to take these findings in detecting different types of leukemia earlier and ideally to prevent the complication. This is a fundamental step to estimate the burden of blood cancer and to understand how the occurrence of this disease varies according to clinical features, morphological types, gender, age, laboratory parameters of this hematological malignancy.
Materials and Methods
Patients
This retrospective study was performed on 98 patients out of 1,20,500 patient diagnosed with leukemia from the Department of Pathology, during May 2018 to April 2020. These patients were evaluated especially regarding clinical features, morphological types, gender, age at diagnosis, haematological findings.
Exclusion criteria
All persons coming for medical fitness.
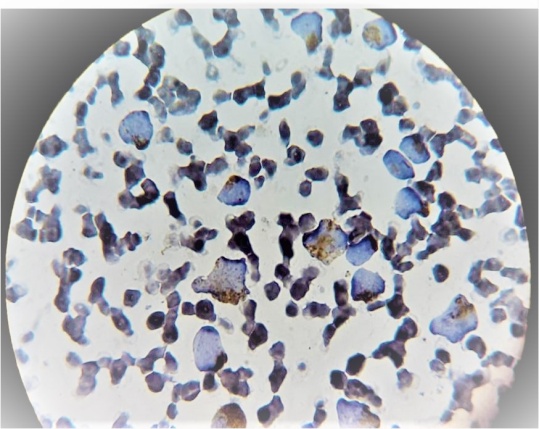
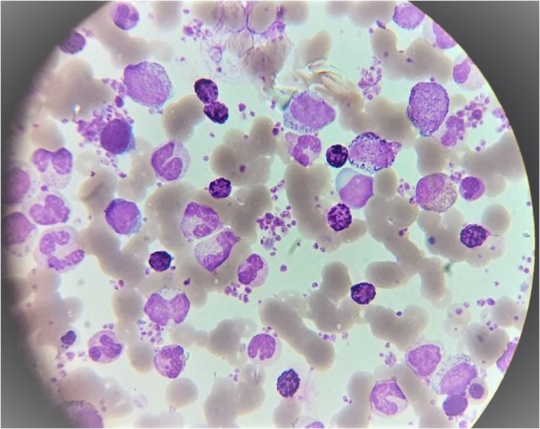
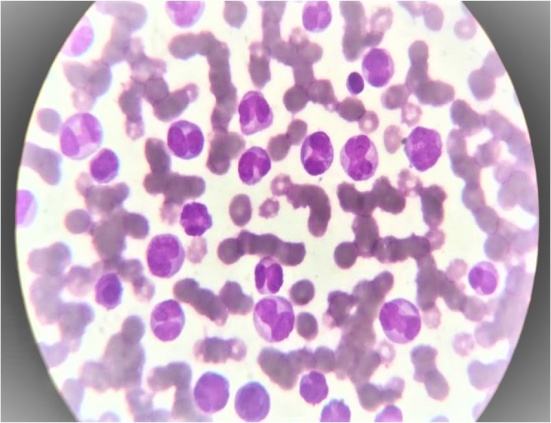
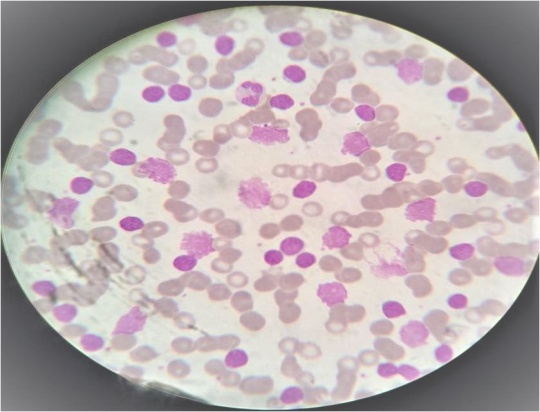
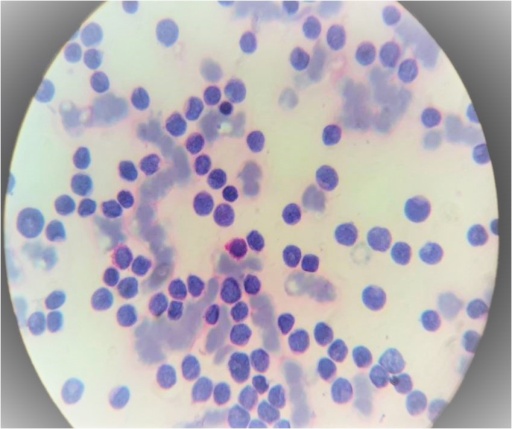
The whole blood samples of patients were taken with informed consent for haematological analysis. Haematological parameters were measured using cell counter NIHON KOHDEN MEK9100K and by microscopical examination. Slides were prepared with PBF (Peripheral Blood Film) by using ‘Routine stain and special stain’ to find out the blast cells morphology in peripheral blood sample of all patients of blood cancer. Diagnosis of leukemia was done by 20% blast criteria and then Special stain (MPO&PAS) were used to distinguish between AML & ALL. Morphological subtyping was done according to the French-American-British (FAB) classification using morphological and cytochemical criteria to characterize the blast cells. The distribution of cases of leukemia was studied according clinical features morphological types, gender, age, haematological findings.
Results
In present research, 98 cases with leukemia out of 1,20,500 (Indoor&Outdoor) cases were analysed during the period from May 2018 to April 2020.
Results according to clinical features
The majority of our patients were presented with low grade fever, progressive pallor, generalized weakness, anemia and bodyaches. Lymphadenopathy is more common in ALL. Hepatosplenomegaly was commonly seen in patients of AML and CML.
Results according to morphological types
Acute leukemias (57.2%) are more common then chronic(42.8%). AML (36.7%) is more common followed by CML(30.6%), ALL(20.4%) and CLL(12.2%).
Result according to gender
There were 55.4% male patients and 44.6% female with acute leukemia. There were 60% male patients and 40% female patients with chronic leukemia. Among four major type of leukemia, AML in 19% male and 17% female patients, CML in 19% male and 11% female patients and CLL in 6% male patients and in 6% female patients, ALL in 12% male and 8% female patient.
Results according to age
Acute lymphocytic leukemia (ALL) was more commonly noted in children (<15 years) whereas AML was more commonly noted in adults (>15 years). Both CML and CLL were observed only in adults.
Result according to haematological findings:


Table 1
Various morphological types of leukemia
|
Acute Leukemia |
Chronic Leukemia |
|
ALL (20.5%) |
CLL (12.2%) |
|
AML-M0 (6.1%) |
CML (30.6%) |
|
AML-M1 (6.1%) |
|
|
AML-M2 (10.2%) |
|
|
AML-M3 (8.2%) |
|
|
AML-M4 (6.1%) |
|
Table 2
Age wise distribution of various types of leukemia
|
Gender |
AML |
ALL |
CML |
CLL |
|
Male |
19% |
12% |
19% |
6% |
|
Female |
17% |
8% |
11% |
6% |
Table 3
Median age in various types of leukemia
Table 4
Various parameters in various types of leukemia
|
Parameters |
AML |
ALL |
CML |
CLL |
|
Mean haemoglobin(gm/dl) |
8.5 |
4.5 |
6.8 |
6.3 |
|
Mean total count(/cumm) |
44,000 |
45,000 |
2.0 |
95,000 |
|
Mean platelets count(lacs/cumm) |
1.7 |
20000 |
3.0 |
2.7 |
|
Median blast cell(%) |
45 |
42 |
18 |
15 |
Table 5
Comparision of clinical features of leukemia
|
|
Present study(%) |
Study by Radha Rathee et al.8 (%) |
|
Fever |
77 |
89.15 |
|
Pallor |
65 |
77.57 |
|
Bodyache |
62 |
72.08 |
|
Generalized weakness |
70 |
72.45 |
Table 6
Comparison of various parameters of leukemia
|
|
Present study |
Study by Radha Rathee et al.8 |
|
Median age(year)AML, ALL |
28&03 |
28&22 |
|
Median age(year)CML, CLL |
36&58 |
26&58 |
|
Mean haemoglobin(gm/dl) AML, ALL |
8.5&4.5 |
8.5&7.5 |
|
Mean haemoglobin(gm/dl) CML, CLL |
6.8&6.3 |
6.8&6.3 |
|
Mean total count(/cumm) AML, ALL |
44000&45000 |
44000&70000 |
|
Mean total count(/cumm) CML, CLL |
200000&95000 |
140000&52000 |
|
Mean platelets count(lacs/cumm) AML, ALL |
1.7&15800 |
57000&65800 |
|
Mean platelets count (lacs/cumm) CML, CLL |
3.0&2.7 |
1.3&2.5 |
|
Median blast cell (%) AML, ALL |
45&42 |
45&38 |
|
Median blast cell (%) CML, CLL |
18&15 |
42&35 |
Discussion
Haematological malignancies are common in our country. Different studies have been conducted on various aspects of individual haematological malignancies in the past. Many workers have compiled information on haematological malignancies in India.1 In present study acute leukemia (68%) was more prevalent as compare to chronic type (32%) and similar findings have been reported by [3-Radhee] study. In our study, commonest type of leukemia was AML and CML followed by ALL and CLL, studies by [3-Radhee] reported the same. We found a male preponderance in our study. This has also been reported by earlier studies [1,6- Chaudhari S, Kumar A]. Increased incidence of all leukemia in males seems to arise as males are comparatively more exposed to occupational and environmental carcinogens as has been suggested by[1,6- Chaudhari S, Kumar A]. The leukemic blasts in the peripheral blood was highest in the AML with a median blast cell count (45%) followed by ALL (42%), CML (18%) and CLL (15%). These findings were also comparable with studies by [6- Kumar A]. It was observed that low grade fever (77%), progressive pallor(63%), generalized weakness (70%) and bodyaches (62%) were the most frequent symptoms, while pallor was the most frequently found sign in AML&ALL and hepatosplenomegaly was noted most frequently in AML&CML. Our findings are not much different from the earlier studies by[7-Advani SH]. These findings can be explained by the mechanism of leukemia as a maturation block and/or suppression of erythroid and megakaryocytic cells by increased production of blast cells resulting in defective/decreased production of normal leucocytes(fever), erythrocytes(anemia/pallor).
Conclusion
Present study revealed that Acute leukemia was more prevalent than chronic leukemia. The most common type of leukemia was AML followed by CML, ALL and CLL. Overall leukemia was more commonly seen in male patients. Age has significant effect on type of leukemia. ALL was more commonly observed in children whereas both CML and CLL were only observed in adults. Most of the CLL cases were diagnosed accidently when patient come for routine blood check up. The incidence of AML was higher in adults as compare to children and decrease towards older age. The majority of patients had lower haemoglobin, high leukocyte count and lower platelet count, low grade fever, progressive pallor, generalized weakness, anemia and bodyaches. This study is useful for earlier diagnosis of patients with leukemia, so patient get treatment earlier and we can prevent complication. Some types of leukemia respond well to the treatment, and many patient can be cured. There were a no. of limitation of our study. It was a retrospective, hospital based study. There was selection bias as all cases were the ones which presented to hospital. Hospital based study also does not account for the no. of similar cases in the community, therefore, the estimate of relative prevalence can not be generalised. There was no confirmation of diagnosis by flow cytometry, immunohistochemical and cytogenetics studies and there was no follow up of patient to monitor prognosis.