Introduction
Peripheral ossifying fibroma is a focal, non-neoplastic lesion and usually classified as a reactive hyperplasia of gingiva. It is derived from the cells of periodontal membrane. Females are affected more commonly than males and may arise as a result of trauma or irritation caused by ill fitting dentures, plaques or calculus.1 Hormonal influence also has been considered as etiopathogeneis.2 Clinically it presents as a painless solitary mass. It is slow growing mass which may be sessile or pedunculated. The surface is smooth or sometimes with ulceration and the colour appears as pink or red.2, 3 Clinically, it is difficult to distinguish from other reactive lesion of gingiva such as pyogenic granuloma, giant cell fibroma or peripheral giant cell granuloma.3 Hence histopathological confirmation is needed because POF has high recurrence rate.
Case report
A 15 year old girl presented to dental outpatient department with chief complaint of painless growth of gingiva which progressively increased in size. There was no relevant medical and family history. Patient did not give any history of trauma.
On intraoral examination, a pedunculated growth was seen in gingiva in relation to 21,22,23 which measured about 1x 0.5 cm. Mass was bright red in colour with smooth surface. No secondary changes such as ulceration or fungation seen. On palpation it was firm in consistency with mild bleeding on probing. The provisional clinical diagnosis of traumatic fibroma was made.
After getting consent from the patient’s parents, patient was subjected to excisional biopsy under local anaesthesia and the excised tissue was sent for histopathological examination.
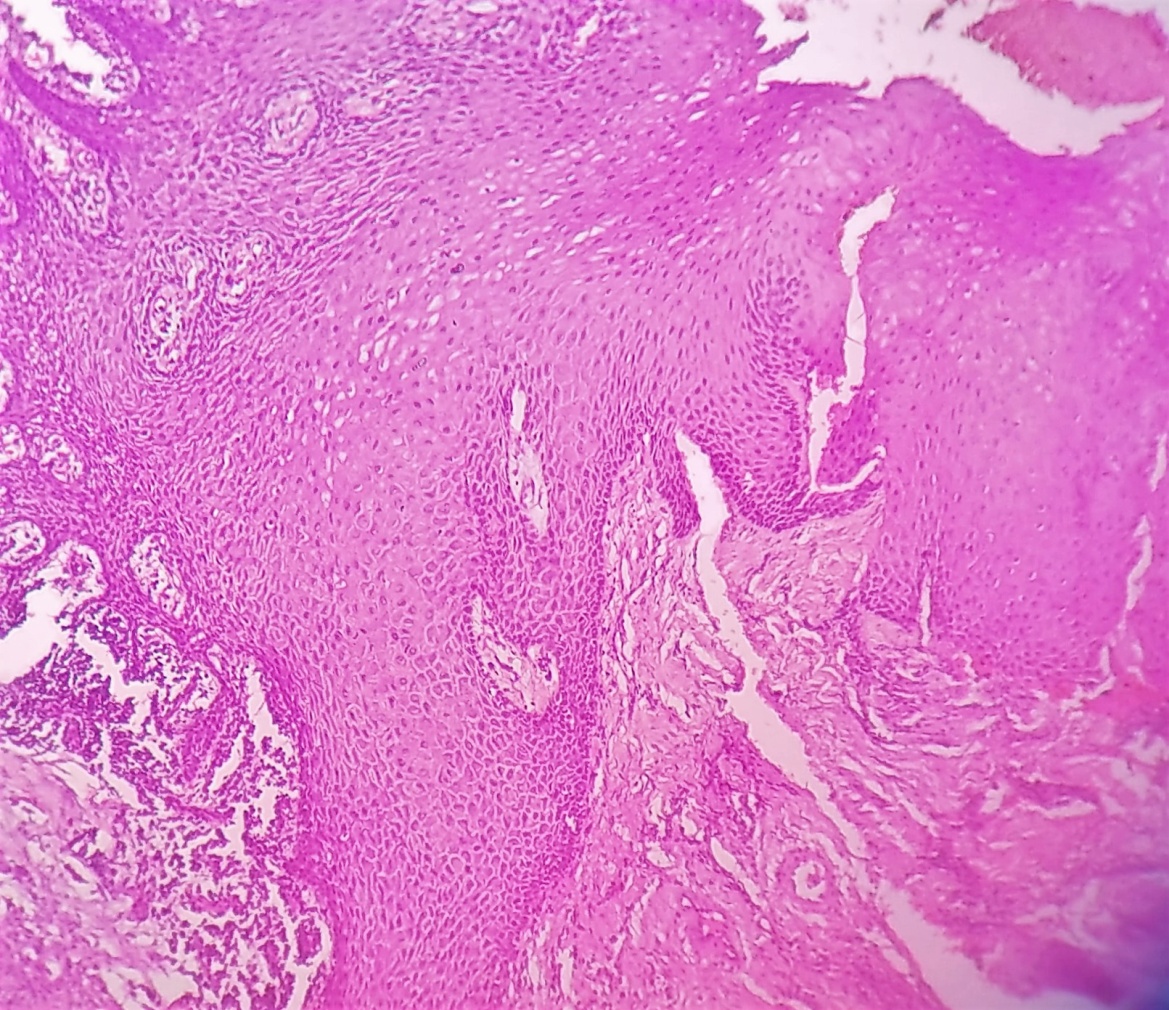
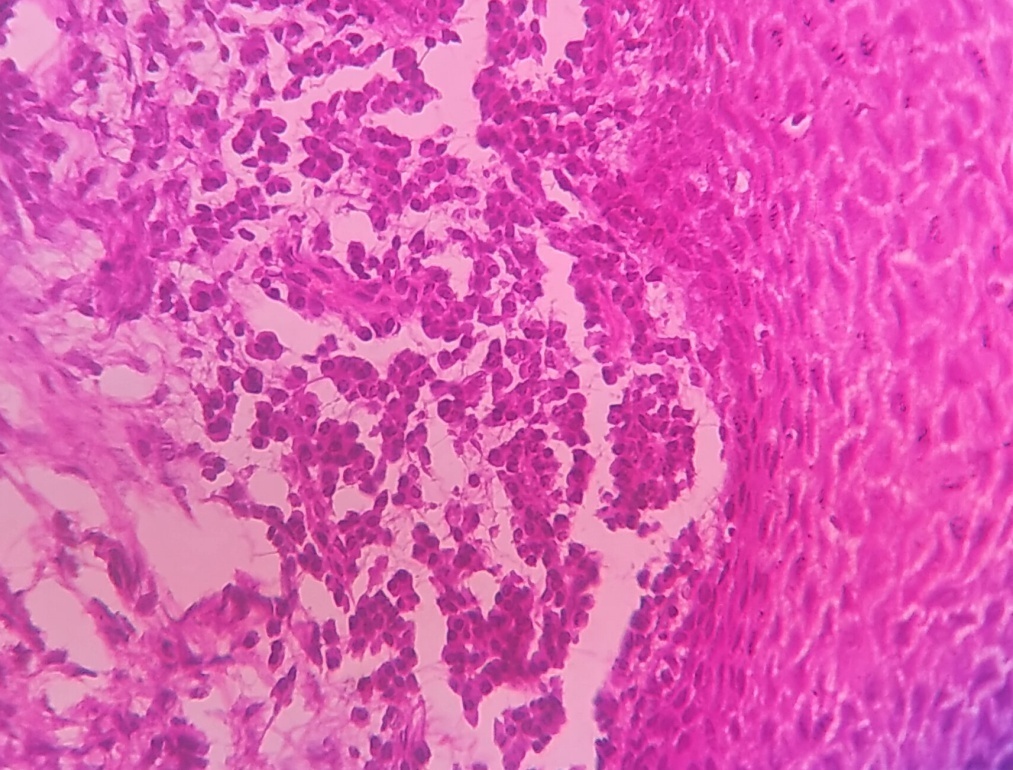
The specimen consisted was a grey white nodular mass which measured 0.8x 0.5 cm and firm in consistency. The specimen was cut into two halves and the whole specimen was submitted for tissue processing. Histologically, tissue section revealed hyperplastic stratified squamous epithelium with focal area of ulceration and granulation tissue formation. Subepithelium showed dense chronic inflammatory cell infiltrate along with areas of ossification and cementum like material embedded in a dense fibrous stroma. (Figure 1, Figure 2, Figure 3).
On the basis of patient age, clinical presentation and histopathological features, the final diagnosis was given as peripheral ossifying fibroma.

Discussion
Gingiva is one of the commonest location in oral cavity, presents with variety of lesions ranging from inflammatory to neoplastic.1 In that, POF is one of the non neoplastic reactive lesion which constitutes about 10-18% of all gingival growth.2
POF was first reported by Stepherd in the year 1844 as “alveolar exostosis”.4 Later, Eversol and Robin coined the term Peripheral ossifying fibroma in 1972.2 It commonly occurs in younger age group with female predilection of 1.3 to 1.7 times than males.5, 6 In literature, it has been known by different synonyms such as peripheral cementifying fibroma, calcifying or ossifying fibroid epulis and peripheral fibroma with calcification, peripheral cement ossifying fibroma.1, 2
Almost 60% of growth have been reported in maxilla and more than 50% involves incisor cuspid area and less commonly premolar region will also be involved.5, 6 POF occurs most commonly in second decade, as age advances there will be loss of periodontium accompanying tooth loss so the incidence will be low.1, 2, 6
Clinically, it presents as a solitary, slow growing mass. It can be sessile or pedunculated, usually non tender and firm in consistency on palpation. The colour of the lesion may appear as red or normal colour as surrounding mucosa.7, 6, 8 In literature, most of the lesion reported by Kfir et al. is usually less than 1.5 cm in diameter but size upto 9cm has also been reported.2 Clinically it has many differential diagnosis, hence histopathology is confirmatory.
Radiography usually shows no involvement of underlying bone. Occasionally there can be superficial erosion of bone and loosening of adjacent tooth.2 The histogenesis of POF is uncertain, Eversole and Rovin as well as Bhaskar and Jacoway suggested that it is a inflammatory hyperplasia of periodontal membrane.1, 2, 3, 8 Other causes such as ill fitting dental appliances, dental calculus, plaques and hormonal influence could be responsible for POF.8, 9 Microscopically it is composed of proliferation of bland fibroblasts with a collagenous stroma covered by stratified squamous epithelium. The stroma contain dystrophic calcification and reactive bone.2, 3 The treatment of choice is surgical excision and high recurrence rate due to incomplete excision occur.1, 2, 3, 10
Conclusion
Peripheral ossifying fibroma is a slowly progressing reactive lesion of gingiva. Even though a nonneoplastic lesion, it is mandatory to diagnose by histopathological examination as other reactive lesion also have similar clinical presentation. At the same time, its high recurrence rate of 8-20% should prompt complete surgical excision and follow up of the patient.
Acknowledgement
We would like to acknowledge the patient and her family for allowing us to use her medical records in our case report and allowing the case to be published.
Availability of Data and Materials
We respect the patients rights to privacy and to protect his identity, so we do not wish to share our patient data. We presented in the manuscript, all the necessary information about the case report. Raw data regarding our patient in her admission file, a file that is strictly confidentaila, without the possibility of publishing raw data from it.