Introduction
In 1782 Wardrab coined the term “soft tissue”
Soft tissue is nothing but a nonepithelial extra skeletal tissue of the body without reticuloendothelial system, glia, and supporting tissue of various parenchymal organs. It includes smooth muscles, striated muscles, fat and fibrous tissue, with vessels. It also includes peripheral nervous system because tumors from nerves present as soft tissues masses. Soft tissue is derived embryologically from mesoderm with some contribution from neuroectoderm.1
Benign soft tissue tumors 10 times more common than malignant one. Soft tissue sarcomas compared with carcinomas and other neoplasm, are relatively rare and less than 1% of all malignant tumors.1 They occur in any part of body, most commonly in extrimitis, trunk, abdomen and head and neck.2
Soft tissue tumor and tumor like lesions have very wide variety and c lose histopathologic findings between certain tumors with little difference detect at close examination under microscope, so it appeal to give diagnostic challenge to histopathologist. For e.g. ‘nodular fasciitis ’or‘ atypical lipoma’ which is being misdiagnosed as fibrosarcoma or pleomorphic liposarcoma respectively.
Light Microscopic evaluation of hematoxylin-eosin stained section is still the standard technique for the diagnosis of these tumor malignancies.3 Grading of malignant tumors is the most established criteria for predicting the biological behaviour of these tumors which is not essential to give proper therapy,4 but it is confirmed by immunohistochemistry, cytogenetics and electron microscopy for the precise role diagnosis.5 Special stains in soft tissue pathology plays variable role or inconclusive or to justify the light microscopic diagnosis.6 This variability, diversity and uniqueness of these tumors produce interest of undertaking a study on soft tissue tumors.
Materials and Methods
Four years of study (two years retrospective and two tears prospective) was done from June 2008 to June 2012 in tertiary care hospital. Total 360 Soft tissue tumors were obtained in these four years. We record parameter like age, sex, and anatomical location of tumor from clinical record and history. All these tumors we categorized under extremities, trunk-abdomen and head and neck region.
Gross examination done in detailed with tumor size, consistency, presence of necrosis, haemorrhage, calcification, status of capsule, surgical margin of resection and invasion or adhesion of tumor to the adjacent structures.
Several sections were taken and stained with haematoxylin and eosin. Detailed microscopic analysis was done including type of tumor cell, arrangement, and pleomorphism. Also examined for necrosis, mitosis, lymphovascular embolism, haemorrhages. Special stains like orcein, reticulin, PAS, Masson’s trichrome and PTAH were conducted wherever necessary.7
Immunohistochemistry was done in 15 cases. Markers used are vimentin, cytokeratin, desmin, neurofilament protein, EMA, Myoglobin, CD31, CD34, BCL2, S100 and SMA. The tumors were classified according to WHO classification.8
We include benign and malignant soft tissue tumors of various parts of body, except uterine and gastrointestinal soft tissue. Tumor like lesion also excluded.
A chi-square test was used, which showed that these results were statistically significant.
Results
From entire surgical material (18134 cases) soft tissue tumors was 1.9%(360 cases) in 4 years duration.[Figure 7]
Soft tissue tumors represented 9.9% (360 cases) of all tumors (3650 cases) received during these four years study. [Figure 8]
91.7%(330 cases) formed bulk of benign soft tissue tumors while 8.3%(30 cases) formed malignant one.
Ratio of benign to malignant soft tissue tumor is 11:1 in this study.[Figure 9]
The highest prevalence of benign soft tissue tumors was in third decade while malignant tumors had in fifth decade.[Table 1]
Soft tissue tumors had slightly male preponderance having male to female ratio was 1.3:1. Male to female ratio in benign tumors was 1.2:1 and among malignant tumors ratio was 2:1 [Table 2]
Extremities were the commonest location for both benign and malignant soft tissue tumors there after head and neck region was common. [Table 3]
The most common benign tumor in this study was lipoma (52.4%) form all benign tumors followed by vascular tumors (21.2%), peripheral nerve sheath tumors (20.9%), fibrous tumors (3.3%), fibrohistiocytic tumors (1.8%) smooth muscle tumors and tumors of uncertain differentiation(0.3%) in descending order.[Table 4]
Among the malignant soft tissue tumors liposarcoma (33.3%) was commonest, followed by malignant peripheral nerve sheath tumors, angiosarcomas, rhabdomyosarcoma (13.3%). Leiomyosarcoma and malignant fibrous histiocytocytoma(10%), synovial sarcoma (6.6%) in descending order of frequency.[Table 4]
Special stains like PTAH, PAS, and reticulin were useful in some problematic cases as well as highlight some structures for learning purpose.
In present study 30 malignant tumors were graded according to FNCLCC grading system as follows-
Grade I: 13
Grade II: 10
Grade III: 07
Immunohistochemistry for tissue-related marker has proved of great value & is now widely used for accurate classification of these neoplasms.
We did IHC on 15 cases. In 10 cases the histopathological diagnosis was confirmed on IHC. 3 cases we diagnosed as high grade sarcoma which were we further classified them on the basis of IHC findings. 2 cases had difference in light microscopic and IHC findings.
Discussion
Soft tissue tumors are very rarely obtained samples in histopathology department. In our study we received 360 soft tissue tumors; we recorded clinical data which includes age, sex, and location of tumor. Along with also record the incidence and different microscopic pattern of soft tissue tumors. We have compared our results with similar studies in India and abroad. Thus data available for comparison is from different geographic areas and of different time periods. Collective studies of all types of soft tissue tumors are very few as compared to individual soft tissue tumor.
In our study soft tissue tumors accounted 9.9% of all tumors from which 9.04% are benign tumors and 0.82% constituted by malignant tumors.
Total 360 soft tissue tumors are studied, 330 are benign while 30 are malignant in present study constituting 91.7% and 8.3% respectively. Benign to malignant ratio is 11:1 in our study, which is comparable to study done by Myher Jensen et al9 1981 who reported ratio 18:1. M.J. Kransdorf et al10,11 in 1995 reported ratio 1.5:1, Lazim et al12 in 2008 reported as 5.1:1, Bashar et al2 in 2010,and Beg et al13 in 2012 also reported a benign to malignant ratio as 3:1,and 5:1 respectively. These studies also comparable with our study. [Table 5].
Soft tissue tumors found more often in male than female, ratio is 1.3:1 in present study, which is similar to Myher Jensen et al9 1981, M J Kransdorf et al10,11 1995, Beg et al13 in 2012 reported an incidence as 1:1,1.2:1, and 1.8:1 respectively. [Table 6]
In present study age ranged from 2 months to 72 years and 35.5 years is the average age of benign tumors which is comparable with studies done by Myher Jensen et al9 1981, Bashar et al2 in 2010 and Agravat et al14 2010 reported average age 44.5, 27.6, and 26.6 respectively. The average age of malignant tumors is 47.7 years which is similar to studies done by Myher Jensen et al9 1981, Bashar et al2 in 2010, Agravat et al14 2010, Lazim et al12 in 2008, and Peterson et al15 2011 reported average age 49.5,39.1,64,30.5, and 63 years respectively.[Table 7]
In our study commonest site of benign tumors is an extremity (33%) mainly lower extremities, followed by head and neck region (32.1%), which is comparable with Beg et al in 2012 stud y showing common location of benign tumors in extremities (40.9%) then head and neck (35.5%).13 M.J. Kransdorf et al 1995 also reported the same site incidence as 60.6% in extrimities, 13.8% in head and neck.10,11
In present study malignant tumors frequently observed in extremities (60%), mainly lower extremities which is followed by trunk and abdomen (23.3%) which is similar to M.J. Kransdorf study.10,11 Also comparable with Lazim et al12 in 2008, Zhi-wei et al,16 Beg et al.13
Lipoma (52.4%) is the commonest benign tumor found, followed by hemangioma (21.2%) and schwannoma (20.9%) which is comparable to Myher Jensen et al9 1981 and M.J. Kransdorf study10,11 1995.
The commonest malignant soft tissue tumor is liposarcoma (33.3%), followed by malignant peripheral nerve sheath tumors, angiosarcoma, rhabdomyosarcoma (13.3%), leiomyosarcoma and malignant fibrous histiocytoma (10%), synovial sarcoma (6.6%) in descending order of frequency which is similar to M.J. Kransdorf study10,11 1995.
Figure 1
Well differentiated liposarcoma- Thickened fibrous septa that display large hyperchromatic cells (H& E, X400) with gross finding
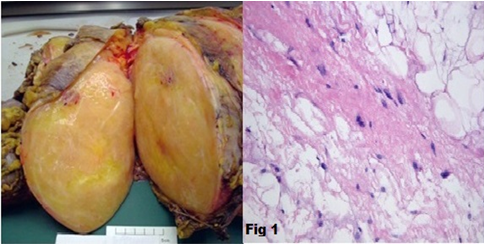
Figure 2
Myxoid liposarcoma – mixture of uniform round to oval cells with signet ring lipoblasts in prominent myxoid stroma along with “chicken wire” capillary vasculature (H & E, X400) with gross finding.
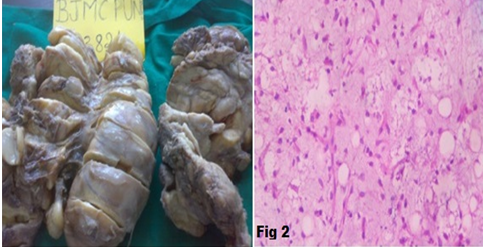
Figure 3
Pleomorphic liposarcoma showing pleomorphic spindle cells with pleomorphic multivacuolated lipoblasts with bizarre hyperchromatic and scalloped nuclei. (Arrow showing pleomorphic lipoblast) (H & E, X400) with gross finding.
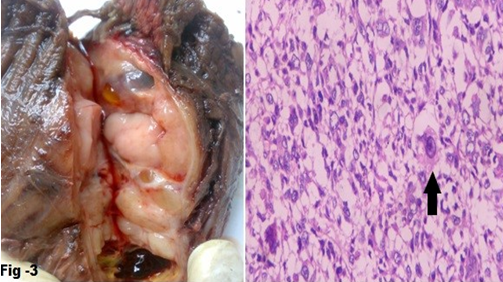
Figure 4
MPNST- Tightly packed spindle cells arranged in fascicles with elongated nuclei with eosinophilic cytoplasm and brisk mitotic activity (H & E, X400) with gross finding
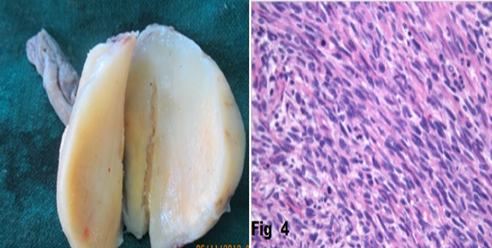
Figure 5
Synovial sarcoma (monophasic pattern) with diffuse positivity for bcl2 (In Inset) (H & E, X400, IHC, X400)
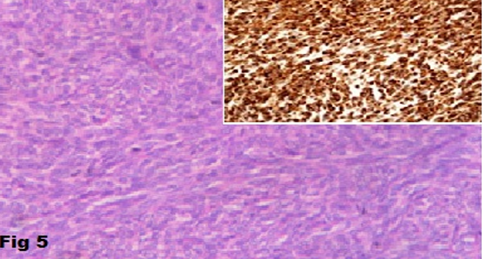
Figure 6
Pleomorphic rhabdomyosarcoma (high grade) with myoglobin positivity (In inset) (H & E, X400, IHC, X400)
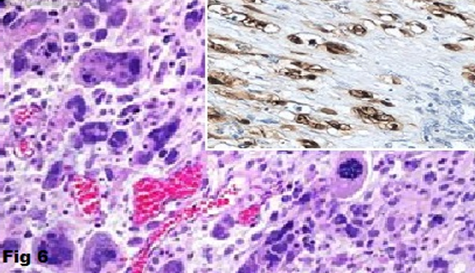



Table 1
| Age in yrs | Sex | Total | |
| Male | Female | ||
| 0-10 | 11 | 16 | 27 |
| 11-20 | 31 | 23 | 54 |
| 21-30 | 44 | 32 | 76 |
| 31-40 | 34 | 35 | 69 |
| 41-50 | 33 | 24 | 57 |
| 51-60 | 25 | 15 | 40 |
| >61 | 23 | 14 | 37 |
| Total | 201 | 149 | 360 |
Age & sex incidence in soft tissue tumors
Table 2
Sex Incidence of all SSTS
Table 3
| S. no | Site | Benign | Malignant | Total |
| 1 | Extremities | 109 | 18 | 127 |
| 2 | Head and Neck | 106 | 04 | 110 |
| 3 | Back and Shoulder | 76 | 01 | 77 |
| 4 | Trunk and Abdomen | 35 | 07 | 42 |
| 5 | Others | 04 | 00 | 04 |
| 6 | Total | 330 | 30 | 360 |
Site distribution of Benign and Malignant soft tissue tumors
Table 4
Incidence of benign and malignant soft tissue tumors
Table 5
Comparative analysis of incidence of benign and malignant soft tissue tumors
Table 6
Comparative analysis of sex ratio of all soft tissue tumors
Table 7
Comparative analysis of age incidence of benign and malignant soft tissue tumors
Conclusion
Soft tissue sarcomas occursrarely, presented as painless mass, so it should be diagnosed quickly for the sake of better management and good prognosis of patients. Diagnosis and management is a team work of clinicians and pathologist.
Careful gross examination with appropriate sampling of soft tissue tumor is essential. New advance techniques like special stains, immunohistochemistry, and molecular studies are useful in addition to routein light microscopic findings for exact diagnosis. But higher cost of these tests is the main limitation.
Clinicopathological correlation is still the gold standard for correct diagnosis of soft tissue tumors in the centres where the advance techniques are not available.