Introduction
Cholecystectomy is one of the most frequently performed emergency abdominal operation as the gallstones are one of the major causes of morbidity and mortality all over the world affecting 10% of adult population.1 Cholecystectomy specimens are mostly associated with gall stone called as calculous cholecystitis, and because of westernization of life style incidence of gall stones is increasing in India. Hence, gallbladder is a frequent surgical specimen in most of the histopathology laboratories.
According to consolidated report of population based registries of India 2009-2011 (by National centre for disease informatics and research), India has shown high incidence of gall bladder cancer in female population of Kamrup (Assam) district, which is highest among the world.2
Clinical diagnosis of the cholecystitis is made, based on history and physical examination along with laboratory and radiological findings. However, histopathological study is the gold standard for the diagnosis of cholecystitis. Histopathological examination many time reveals an unusual diagnosis bearing significant implications on the treatment, prognosis and outcome of the patient. Hence, present study was undertaken to emphasize the role of histopathological examination in cholecystectomy specimens and its correlation with clinical presentation.
Aim and Objectives
To study various lesions encountered in cholecystectomy specimens on histopathology.
Materials and Methods
Source of data
The present study includes prospective cases of two years from June 2015 to May 2017 and also includes cases from retrospective archival of data of two and half years i.e. – Jan 2013 to May 2015. Thus it includes 130 cases of cholecystectomy specimens during Jan 2013 to June 2017.
Inclusion criteria
All Cholecystectomy specimens received in the department of Pathology in our institute during Jan 2013 to June 2017.
Method of data collection
The specimens were collected in 10% formalin following scrutiny of the patient details and identity. The specimens of cholecystectomy were fixed in formalin for 12-24 hours. Gross examination of all the specimens were done. Bits from one representative full-thickness section from the fundus, one through the body, one through neck of the gallbladder, and one cross section of the cystic duct margin were taken. Additional sections were taken when focal lesions were present. These were followed by routine paraffin processing.
Observations and Results
Out of these 130 cases, in 129 (99.23%) cases gall bladders was surgically resected as a therapeutic measure for clinically suspected cholecystitis and in remaining only 1 case (0.77%) gall bladder was removed with Pancreaticoduodenectomy.
Out of 130 cholecystectomy 111 were laproscopic and 19 were open laprotomy cholecystectomy.
Out of 19 open laprotomy procedures 2 procedures were initially started as laproscopic cholecystectomy and were converted in to open procedures as gall bladders having necrotizing cholecystitis got ruptured during procedure.
Maximum numbers of patients were in the age group of 41-50 years (26.1%) followed by 51-60 years (20.8%) and 61-70 (18.4%) years.
Mean age of the patient was 50 years. Oldest patient was 80 years, and the youngest was 17 years of age.
Females were common in age group of 31 to 60 years. After 60 years male patients were more common.
Table 1
Distribution of cholecystectomy specimens according to histopathology diagnosis
Figure 1
Photograph showing specimen of s hrunken gallbladder with chronic cholecystitis. Lumen is filled with bile and single pure cholesterol stone

Figure 2
Photograph showing specimen of gallbladder with gangrenous cholecystitis case, showing severely congested serosa

Figure 3
Photograph showing specimen of gallbladder with acute cholecystitis showing swollen enlarged gallbladder with congested serosa and thickened wall. Lumen shows congested mucosa and mucosal ulceration

Table 2
Histopathological diagnosis and presence of gall stones
Out of 107 cases of chronic cholecystitis 99 (92.5%) were calculous cholecystitis and 8 were acalculous cholecystitis.
Out of 12 cases of acute cholecystitis 8(66.6%) were calculous cholecystitis and 4 were acalculous cholecystitis.
Out of 4 cases of carcinoma specimens 1 showed calculous.
Table 3
Analyses of gallbladder carcinoma specimens
Table 4
Histopathological examination and outcome of gallbladder carcinoma patients
Out of total 130 cases, 4 (3%) patients of gall bladder carcinoma-
1. Youngest patient was 40 years old and oldest was 65 years old.
2. On ultrasonography Case No.1 showed diffuse wall thickening and Case No.4 was diagnosed as polyp. Case No. 2 and 3 were diagnosed as gallbladder carcinoma, but diagnosis of malignancy was missed on USG in Caes No.1 and Case No.4.
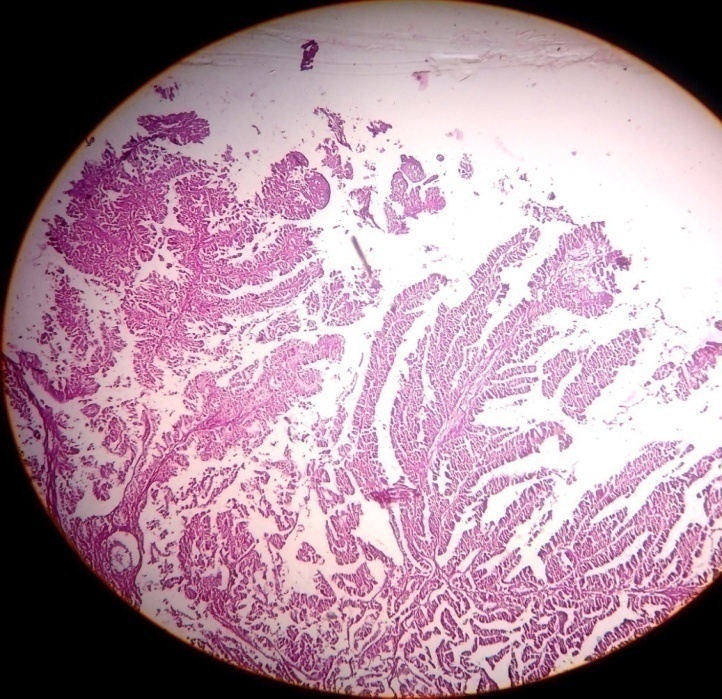
3. Case No. 2 was well differentiated papillary carcinoma, Case no. 3 was of poorly differentiated adenocarcinoma and Case No. 1 and 4 were well to moderately differentiated adenocarcinoma.
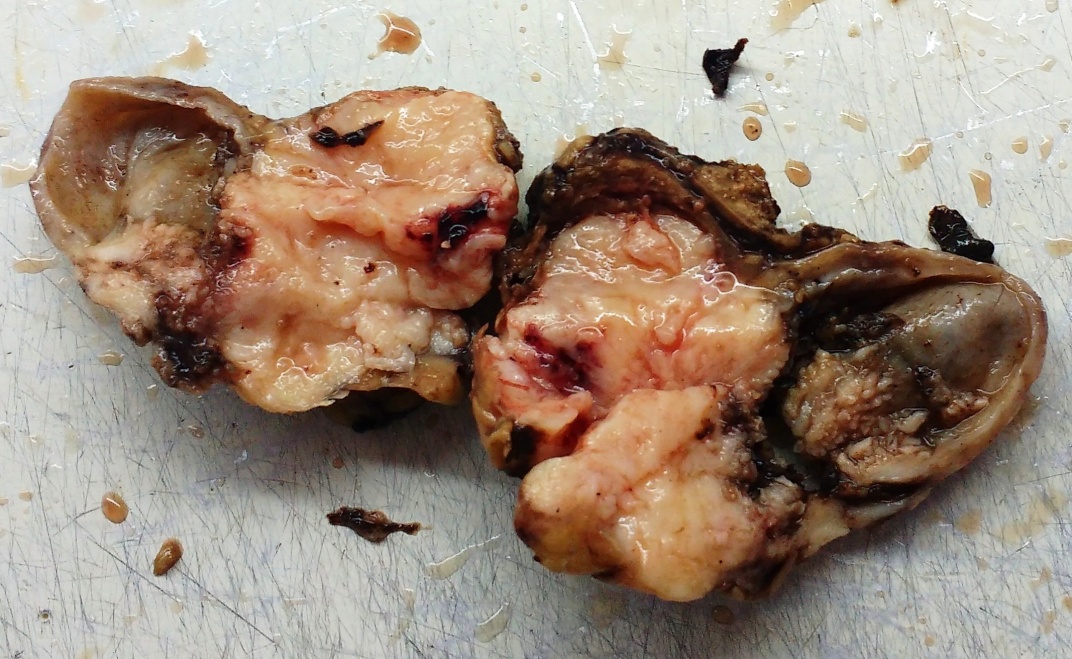
Figure 4
Photograph showing specimen of gallbladder carcinoma with diffuse gallbladder wall thickening and ulceration of mucosa

Figure 5
Photograph showing specimen of gallbladder carcinoma with growth replacing body and neck and infiltrating serosa
Outcome and duration of hospital stay
Out of Total 130 Cases –
Improved- 127 cases
Espired due to gall bladder disease
2 cases (both were carcinoma of gallbladder. Out of 4 cases of gall bladder carcinoma 2 cases expired in postoperative period)
Expired due to other cause- 1 case (due to periampullary adenocarcinoma)
Average days of hospital stay after laproscopic surgery – 5.4 days.
Average days of hospital stay after laprotomy (open) surgery - 11.00 days.
Discussion
Findings of age and sex distribution in this study are in concordance with studies of Daniel Mønsted Shabanzadeh et al,3 Vikash Talreja et al,4 Yen-Chun Chen et al,5 Tadashi Terada.6
While most of the chronic cholecystitis were calculous (in present study 89.7%), there was no significant difference noted in gross as well as histological features of chronic calculous cholecystitis and chronic acalculous cholecystitis. According to literature also its doubtful to call stone as direct etilogical factor for chronic cholecystitis, rather these both processes; formation of stone and development of chronic inflammation are parallel processes due to chronic supersaturation of bile and stasis.7
In the present study acute cholecystitis comprises 9.2% of total cholecystectomy cases. This finding matches with the study of Damor NT et al,1 Vikash Talreja et al.4 Incidence of acute cholecystitis varies round the globe, but still it remains the second most common cause of gallbladder pathology after chronic calculous cholecystitis.
Table 5
Comparison of type of cholelithiasis among received cholecystectomy specimens with other studies
In present study out of total 130 cases 113 (86.9%) had gallstones this finding is in concordance with study of R. Thamil Selvi et al8 and Tadashi Terada.6
Gallstones are directly responsible as a etiological factor in only acute calculous cholecystitis, as the stone inside lumen; in gallbladder neck or in cystic duct obstructs flow of bile. That obstruction and accumulation of bile causes ischemia to mucosa due to pressure effect as well as it causes chemical injury to mucosa because of prolonged stasis of bile in lumen.
Out of total 113 (86.9%) gallstones–4 (3.5%) were pure cholesterol stones, 14(12.4%) pigmented stones, 95 (84.1%) were mixed stone. Findings are in concordance with Pradhan SB,9 Dattal DS et al.10
High serum bilirubin values with pigment stones are predominant in children with hemolytic diseases, but in present study no such case was observed.
Most of the gallstones in north India are cholesterol stones (80%) while in south India they are pigmented (60%).
Appearance of cholesterol gall stones varies with cholesterol content of stone. According to literature pure gallstones account for 10% of total gallstones,11 and they are single, large, oval, and yellowish. Stones with lower cholesterol content are designated as mixed. Depending up on the proportion of calcium carbonate, bilirubin and phosphate mixed stone may be gray yellow to gray black in colour. According to literature also 70-80% stones are mixed stones.11 They are usually smaller, multiple, and faceted.11 In comparison, pigmented stones are multiple, small, black or brown in colour.8
In present study total 89.7% chronic cholecystitis were calculous while 58.3% of acute cholecystitis and 25% of gall bladder carcinoma were associated with stone.
According to literature 70-80% gallbladder cancer are associated with gallstones.12 But in present study gallbladder (GB) stones were found more often in patients with acute cholecystitis than in patients with gallbladder carcinoma. Patients with gallbladder carcinoma showed typical masses or focal enhanced wall thickening when compared to diffuse wall thickening in patients with acute cholecystitis. Findings were in concordance with study of Kim SH13 et al.
In present study out of total 130 cases 107 (82.3%) were chronic cholecystitis. Out of total 107 chronic cholecystitis cases 96(89.7%) were calculous while 8(10.3%) were acalculous. Findings are in concordance with study of Chiam H K et al,14 Vikash Talreja et al,4 R. Thamil Selvi et al.8
Jones-Monahcm K et al15 observed that change from open to laparoscopic cholecystectomy was accompanied by more females undergoing operation for acalculous biliary disease.
Majority of gallbladder with chronic cholecystitis were shrunken with unremarkable serosa. On microscopy gallbladders showed all typical features of chronic cholecystitis like chronic inflammatory infiltration of mucosa, lamina propria. Rokitansky Aschoff sinuses were present in 40(37%) cases of chronic cholecystitis. One caes showed diffuse calcification of gallbladder wall microscopically but grossly specimen was unremarkable.These findings matches with study of R. Thamil Selvi et al8 and Dattal DS et al.10
There was no mortality reported in cases of chronic cholecystitis cholecystitis.
Distribution of different types of pathologies shows chronic cholecystitis (82.3%) was most common finding, followed by acute cholecystitis (9.20%), followed by carcinoma (3%); which are in concordance with Amjad J. Almuslamani et al;16 Ivy Sharma et al;17 Vikash Talreja et al;4 while Tadashi Terada6 found gall bladder carcinoma as more common lesion then acute cholecystitis. But in his study Tadashi Terada6 observed 94% cases as chronic cholecystitis, while only 6% cases are having all other spectrum of gallbladder diseases which is not very uncommon finding.
Gall bladders with chronic cholecystitis were shrunken with unremarkable serosa, where gallbladder with acute cholecystitis and, acute on chronic cholecystitis were swollen and showed exudate and congestion on serosa. Total 3 cases showed perforation, all 3 cases had biliary peritonitis.
Total 113 (86.9%) gallbladder had calculous. In 84 (68.4%) cases gallbladder lumen was filled with bile. In 29(23.8%) cases lumen was filled with mucous and bile, those gallbladders were swollen and congested and had exudate on serosa where diagnosed as acute or acute on chronic cholecystitis. In 4(7.6 %) cases there was presence of growth in lumen and those 4 cases were diagnosed as carcinoma.
The case of Eosinophilic cholecystitis was characterized by predominant infiltrate of eosinophils in the wall of gallbladder. Its etiology was unknown. Conditions like infections, drugs, medicinal herbs, autoimmune disorders, allergy, eosinophilic gastroenteritis, parasitic infestation, hypereosinophilic syndrome, etc. were excluded.
The case of Cholecystitis follicularis was having lymphoid follicles with hyperplastic germinal centers in all layers of gallbladder. Grosly gallbladder had features of chronic cholecystitis. Patient did not have any lymphadenopathy, organomegaly or peripheral blood lymphocytosis. As IHC study is necessary to rule out lymphoma18,19 may be needed in presence of such symptoms.
There were 3 cases of Chronic Xanthogranulomatous cholecystitis. Grossly the specimens were having marked thickening of wall and mucosal ulcerations. Microscopically wall of gallbladders were infiltrated by foamy macrophages in lamina propria and muscularis layers.
Comparison of occurrence of gall bladder carcinoma in various studies around the world shows incidence varies between 0.26% - 3.00%. In the present study it was 3.00%, which was in concordance with study of Archana Tiwari et al;20 Tadashi Terada6 and Romero González. 21
Studies in western countries done by Taylor (1998), Dix (2003), Darmas (2007), Oommen (2007), Bazoua (2007), Byars (2012) of United Kingdom; Romero-González (2012) from Maxico ; Matthyssens (2006) from France and Wolkomir (1991) from US believed that Histopathological examination done post cholecystectomy should be selective and not routine for all cases. As these studies believed on radiological examination as well as intraoperative examination of gallbladder specimen by surgeon could exclude the need of histopathological examination if no suspicion of malignancy on radiological and intraoperative examination.
According to studies in India the highest incidence of gallbladder cancer is in Kamrup district (Assam state), that is 3.5 % of all cancer in males and 8.2% in females. (132 out of 3809 in male and 232 out of 2814 cases in females - total cancer cases study done from year 2007 to 2011). The same study reported high mortality in patients with gall bladder cancer.2
Table 6
Comparison of histological type of gallbladder carcinomas with other studies
Incidental carcinoma is carcinoma which was missed on radiological examination (USG as well as CT) as well as clinical examination of gall bladder intraoperatively and only on Histopathological examination the case revealed to have carcinoma; which is expressed as percentage of total cholecystectomy specimens studied with all different types of pathologies.
In the present study all 4 cases of (100%) malignancy were adenocarcinoma, which is in concordance with, John Patrick Byars;22 K F Chin et al;23 Archana Tiwari et al,20 while Joon Joon Khoo obsereved 78% adenocarcinoma, 11% squamous and 11% adenosquamous carcinoma in his study, and Dinesh Singh et al24 observed 98% adenocarcinoma and 2% squamous carcinoma.
As shown in Table 6, almost all the studies showed majority of carcinoma were ‘moderately differentiated or poorly differentiated adenocarcinomas’.
Association with gall stones was seen in 1 out of 4 (25 %) cases of malignancy; while Dinesh Singh et al,24 Joon Joon Khoo,25 studies showed 55-60 % association with gall stone.
Present study showed that diagnosis of 2 out of 4 (50 %) cases of malignancy was missed on ultrasonography. Instead of reporting as malignancy, ultrasonography findings were reported as diffuse wall thickening and polyp.
Study done by Joon Joon Khoo,25 had missed 78% carcinoma on ultrasonography; John Patrick Byars22 missed 21%; Archana Tiwari et al20 missed 41%; and K F Chin et al23 missed 41% carcinoma cases on ultrasonography.
Present study showed occurrence of incidental carcinoma 1.5%. Study done by Archana Tiwari et al20 showed 1.25% and study done by Joon Joon Khoo25 showed 0.26% incidental carcinoma in their studies.
Study done by Dinesh Singh et al,24 and Archana Tiwari et al,20 showed positive association of malignancy with gallstones and female predominance. Study done by Gupta et al;26 also showed 80 % association of carcinoma with stone and female predominance.
In the present study there was no female predominance and only 1 out of 4 cases of malignancy (25%) were associated with stone, which might be because of low sample size (only 4 cases).
Studies done by Vikash Talreja;4 Dinesh Singh et al,24 showed occurrence of gall bladder cancer in countries like India and Pakistan is relatively early that is before 60 yrs of age (47-57 years); which is in concordance with present study.
In the present study 2 out of 4 cases of malignancy (50%) were male and 2 out of 4 cases of malignancy (50%) were female; but there is female predominance in gall bladder cancer according to other studies. In fact in study of John Patrick Byars;22 100% gallbladder carcinoma patients were female.
Study done by RomeroGonzález,21 found infiltration beyond serosa in 100% cases, while study done by Zhi-qiang Cai27 reported 55.46% cases were positive for liver infiltration. In the present study 3 out of 4 cases of malignancy (75% cases) showed serosal as well as liver infiltration.
Study done by RomeroGonzález21 found jaundice in 66% cases, while study done by Zhi-qiang Cai27 reported jaundice in 22.8% cases. In present study 1 case out of 4 cases of malignancy (25%) showed jaundice, which was high grade adenocarcinoma and patient expired in 15 days of hospital stay.
Conclusions
Results from this study show that variety of gallbladder lesions are observed in cholecystectomy specimens. The most common lesion observed was chronic cholecystitis with cholelithiasis 99 cases (76.1%), followed by acute cholecystitis 12 cases (9.2%). Study showed predominance of female patients between age group 41-50 years. Clinical presentation of diseases of gall bladder is vague. Even malignancy of gallbladder presents late in the course and with nonspecific symptoms, which can misguide the clinicians. Findings of malignancy were subtle on radiological examinations also. Diagnosis of malignancy was made only by histopathological examination (1.5% cases as incidental carcinoma). Hence each and every cholecystectomy specimen must be sent for histopathological examination and studied meticulously, as some unusual findings bearing implications on treatment and prognosis may be seen, regardless of the reason for which cholecystectomy is performed.