Introduction
Spindle cell sarcomas are rare and account for 1-2% of sarcomas. 1 Spindle cell sarcomas are heterogeneous group; include Synovial sarcoma, Fibro sarcoma, Leiomyosarcoma, MPNST, Angiosarcoma.
Cytology is a well established tool for diagnosis of spindle cell sarcomas and it shows high diagnostic sensitivity and specificity for determination of malignancy in soft tissue sarcomas. Role of cytology for documenting recurrent and metastatic lesions is well established. Sub-typing of sarcomas is difficult due to overlapping cytomorphological features.
Grading is the most important prognostic factor and is best indicator of metastatic risk in patients Grading is challenging on cytology especially for spindle cell sarcomas and there are only limited number of studies with variable results.
In this study, we tried to look into cytomorphological features of spindle cell sarcomas that help in sub-typing and attempted to grade them on cytology and to correlate with corresponding grading on histology wherever available.
Materials and Methods
All soft tissue spindle cell sarcomas diagnosed on FNAC from over a period of four year at our Pathology department, were included in the study. Low grade myxoid sarcomas, scanty cellular cases were excluded from study.
May-Grunwald-Giemsa and Papincolau stained smears were examined. Minimum of 4 slides with at least 20 clusters were examined for each case. The sarcomas were subtyped wherever possible. The histopathology was correlated with the help of cell block, biopsy or subsequent resections.
FNAC was performed in a standard manner with 22G needle. Multiple aspirations were attempted from different sites depending on the size of tumor. The material was spread on to slide as a direct smear and the unstained air-dried smears were examined for adequacy. Some of the slides were alcohol-fixed. Air-dried smears were stained with May-Grunwald-Giemsa. Alcohol fixed smears were stained with Papincolau stain. Haematoxylin and eosin stain was used for histopathology slides.
The grading parameters on FNAC given by Weir et al2 are used for this study and they are summarised in Table 1.
Table 1
Grading of spindle cell sarcomas on FNAC
The histopathologic gradin g was carried out using FNCLCC Grading system as given by Trojani et al.3 The parameters for grading included 1. Tumor differentiation, 2. Mitotic count, 3. Tumor necrosis. Each parameter is given scores (one, two, three) and all the scores are summed up to give final histologic grade.
Tumor differentiation
Score 1: Sarcomas closely resembling normal adult mesenchymal tissue (eg, well-differentiated liposarcoma).
Histologic grade
Grade 1: Total score 2, 3
The cytologic and histopathology grade was correlated. A major non correlation between the FNAC and histology grades was defined as a misclassification of low grade (Grade 1) specimen Vs Intermediate (Grade 2) or High grade (Grade 3) specimen. A minor non correlation between the FNAC and histology grades was Grade 2 Vs Grade 3 or vice-versa.
Results
A total of 46 cases of spindle cell sarcomas diagnosed on FNAC are included in the study. These included 30 male and 16 female patients (M:F=1.8:1) in the age range of eight to seventy five years (mean age-36.3yr). The locations for the tumors were lower limb (22), upper limb(five), back(three), retro peritoneum(seven), lymph node(seven).
The histopathology was available in 34 cases. This included cell block (8/34), biopsy (5/34) and resections (21/34).
Diagnosis given on cytology in all the forty six cases is as follows: Synovial sarcoma-17 cases, Spindle cell sarcoma-16 cases, Metastasis in a known case-seven cases, Recurrence in a known case-six cases.
Cytologic Grading was done in all the cases. Number of cases with Grade I is one, Grade II is thirty seven, Grade III is eight. Morphologic diagnosis of Grade I lesion is Spindle cell sarcoma. Grade II lesions included Spindle cell sarcoma, Synovial Sarcoma, Recurrence in a known case, Metastasis in a known case. Five cases of spindle cell sarcoma, one recurrence in a known case and two metastatic cases were Grade III on cytology.
Final Histopathology diagnosis in 34 cases included Synovial sarcoma (twenty), Angio sarcoma(one), Fibrosarcoma(two), Leiomyosarcoma (two), Leiomyosarcoma vs MPNST(one), Leiomyosarcoma vs Synovial sarcoma(one), MPNST(one), Myxo-fibrosarcoma(three), Spindle cell sarcomas (two)
Histopathology grading is done in 33 cases. One case could not be graded due to limited material on cell block. Number of Grade I lesions is three, Grade II is 24, Grade III is six. Morphologic diagnosis of Grade I lesions are Spindle cell sarcoma, Low grade myxofibrosarcoma, Synovial sarcoma. Grade II lesions included Synovial sarcoma-14, Leiomyosarcoma-5, High grade myxofibrosarcoma-1, MPNST-2, Fibrosarcoma-2. One case of Angiosarcoma, three cases of Synovial sarcoma, one case of High grade myxofibrosarcoma, one case of MPNST were Grade III.
The correlation between the cytology and histopathology grading is summarised in Table 2
Table 2
| Histopathology Grading | |||
| Cytology Grading | Grade I | Grade II | Grade III |
| Grade I | |||
| Grade II | 3 (9%) | 22 (66%) | 1(3%) |
| Grade III | 2 (6%) | 5(15%) | |
Cyto-histologic correlation
Concordance rate-27/33 cases (81.8%)
Discordant in 6 cases: Major discordance-3/19; Minor discordance-3/19
All the three Grade I lesions on histology are (spindle cell tumor S-100 focal positivity on biopsy; low grade myxofibrosarcoma on resection; synovial sarcoma on cell block) are Grade II on cytology.
For Grade II tumors (on histology), there was good correlation but for 2 cases which were graded as Grade III on FNAC and Histopathology showed Grade II features.
Possibility of Leiomyosarcoma vs MPNST on cell block; (FNAC from hypochondriac mass which was grade III.)
Possibility of Leiomyosarcoma vs Synovial sarcoma on resection as IHC done does not favor leiomyosarcoma or rule out synovial sarcoma.(FNAC was done from cervical node which was grade III)
All grade III lesions on histology are grade III on cytology except 1 case which was given as low grade synovial sarcoma on cytology
Discussion
FNAC of soft tissue tumors has evolved slowly as effective tool for diagnosis of primary, recurrent and metastatic soft tissue tumors.4 Early and rapid diagnosis is possible on cytology that makes it valuable diagnostic tool, particularly in pre-operative management of soft tissue tumors. Advantages of FNAC are due to low cost of the procedure, low incidence of complications like bleeding and tumor seedling.5,6 Effectivity of FNAC can be improved by multiple aspirations from different sites in accessable mass lesions.7,8
Spindle cell sarcomas are a heterogeneous group including various histopathologic entities like synovialsarcoma, fibrosarcoma, leiomyosarcoma, MPNST, angiosarcoma. Features favouring sarcoma in spindle cell lesions include high cellularity of the smears, nuclear pleomorphism, cellular atypia, presence of mitotic figures and necrosis.
In the present study, 46 cases of spindle cell sarcomas which were diagnosed on FNAC were included. All the benign spindle cell lesions like schwannoma, low grade myxoid sarcomas which turned to be fibromatosis on subsequent histopathology were excluded from the study. Various diagnosis on cytology included: Spindle cell sarcoma (16), Synovial sarcoma (17), Metastasis in a known case of spindle cell sarcoma (seven), reurrence in a known case of spindle cell sarcoma(six). Most common age group was 30-50 yrs. Most common location was lower limb which accounted for 48% of cases.
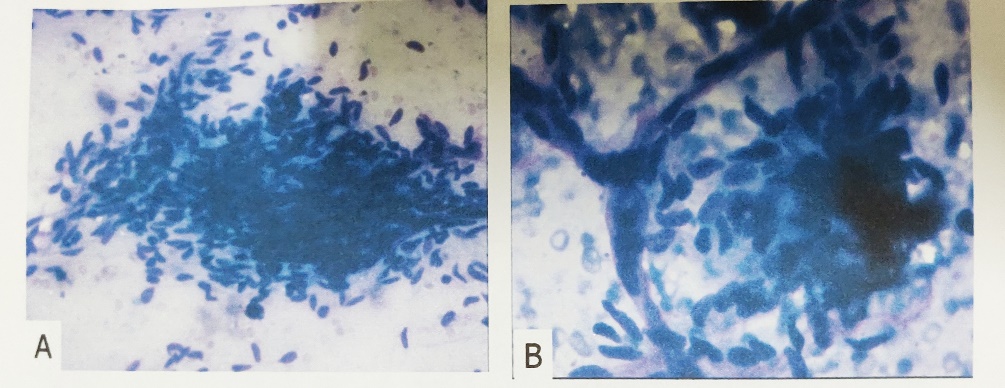
Cytologic features of various spindle cell sarcomas have been well established in the literature. Amongst all the tumors in our study, Synovial sarcomas (17/46) were reliably subtyped on the basis of cytology smears as shown in other studies.9,10 Among seventeen cases, there were four metastatic lesions, one recurrent lesion. Of the twelve primary cases which were diagnosed as synovial sarcomas, the commenst location was lower limb (9/12) and the remaining three cases occurred in upper limb. In primary cases, the diagnosis of synovial sarcoma was given based on cytomorphological features and clinical correlation. Immunocytochemistry was helpful in one case. The features in favor of synovial sarcoma include highly cellular smears made up of densely packed three-dimensional groups and singly scattered oval to spindle cells with bipolar cytoplsmic processes, uniform vesicular nuclei and micronucleoli. Cellular monomorphism and vascular channels within cellular fragments were the remarkable findings. Presence of mast cells and calcification were the additional features (Figure 1). Immunohistochemistry (IHC) showed positivity with Cytokeratin, Vimentin, bcl-2, CD99 and was negative with Desmin, CD34.
Figure 1
(A): Highly cellular- fragments, small clusters and single cells, frayed edges of clusters, vascular pattern (Giemsa 100x) (B): Vascular pattern (Giemsa 200x) C.
In three cases cytology diagnoses offered was 1. Possibility of Fibrosarcoma vs Synovial sarcoma, 2. Synovial sarcoma vs Leiomyosarcoma and 3. Leiomyosarcoma vs MPNST. Differential diagnosis was entertained in these cases due to overlapping clinical and cytomorphological features. Final histopathology was available in first case which turned out to be Fibrosarcoma. IHC showed Vimentin positivity.
There were 3 cases of myxofibrosarcoma in our study. Diagnosis on cytology was myxofibrosarcoma. They included one case of low grade and two cases of high grade myxofibrosarcoma. Two are recurrent lesions of which one was low grade and the other was high grade myxofibrosarcoma. Cytological features evident included myxoid background with numerous curvilinear blood vessels transgressing through cellular clusters
However twenty nine aspirates (29/46) were only diagnosed as Spindle cell sarcomas or Recurrent and Metastatis in a known case. This diagnosis was entertained when specific features of particular sub-type were not convincingly evident on the material studied. The same has been observed in the study by Rekhi et al10 where Only 9/60(15%) cases of spindle cell sarcomas were accurately subtyped and Palmer et al11 where only 9/64(14%) cases were accurately sub-typed.
Complex heterogeneity of SoftTissueTumors is known to be limiting factor in their exact categorization. Appropriate subtyping of each of these tumors is not always possible on cytology only. Clinical and radiological correlation is very much essential before sub-typing. Ancillary techniques like immunocytochemistry can be useful. Exact sub typing of spindle cell tumors is a limiting factor, even in other studies. Kilpatrick et al,12 in their series of soft tissue sarcomas, could accurately sub-type 54% of cases. Various other studies have shown accuracy rates for subtyping ranging from 21-74%.
FNAC is also a valuable tool in the diagnosis of recurrent and metastatic lesions. Recurrent and metastatic cases accounted for 15/46 (32.6%) of all the cases. Majority of the cases were primary in our study as compared to Rekhi et al.10 The reason could be attributed to referal bias. Most common metastatic site included lymph node –inguinal and supraclavicular.
Histologic classification of soft tissue sarcomas has some limitations and is not very convenient for patient care. It is complex, subjected to periodical variations with poor reproducibility.13,14,15 The prognostic value of this histogenetic classification is still under debate. Histologic grading is established as an important prognostic parameter and helps in predicting response to treatment. In a previous study by Coindre et al,16,17 tumor grade was found to be strongly correlated with the advent of metastases and patient survival
Russell et al18 proposed the first coherent and effective system in 1977. The grading parameters included cellularity, cellular pleomorphism, and mitotic activity. Their clinicopathologic classification separated patients into 4 st ages with a different prognosis. It is admitted now that histologic grade is the most important prognostic factor for adult STS and is clearly stated in the World Health Organization classification.1 It should be part of the pathology report along with histologic type and subtype, tumor size, tumor depth, and surgical margins. It should be complemented with radiologic parameters when dealing with a microbiopsy. The most common systems currently used are the French grading (FNLCC)3,19 and the National Cancer Institute grading.20 Both are 3-tier grading systems. In our study, we adopted FNLCC grading system for histology samples.
As fine-needle aspirations are being more widely used in the initial evaluation of primary and metastatic soft tissue tumors, a grading system on cytology for spindle cell sarcomas was developed by Weir et al.2
Various authors have tried to apply grading to FNAC smears of spindle cell sarcomas. 10,13 We tried to grade 46 cases of spindle cell sarcomas on FNAC using three-tier grading system proposed by Weir et al. and to correlate with the corresponding histology grade which was done using FNLCC grading system.Cytology of various grades is shown in Figure 3.
Figure 2
(A): Cytologic Grade I-Singly scaterred spindle cells (Giemsa 100x). Inset showing spindle cells with scant cytoplasm, minimal nuclear atypia and overlap (Giemsa 200x); (B): Cytologic Grade II- Singly scattered spindle cells (Giemsa 100x) with scant cytoplasm, moderate nuclear atypia and overlap; (C): Cyto logic Grade III- Spindle cells with marked nuclear atypia and overlap and prominent macronucleoli (Giemsa 200x).

Majority of cases were grade II (37/46) on cytology. There were 8 (17.3%) grade III cases and only one grade I case. For grade I lesion, final histopathology was not available. Majority (80%) of the cases were called as grade II on cytology as compared to Weir et al.
Final histopathology of lesions which were grade III (7/8) on cytology included Synovial Sarcoma-2, Angiosarcoma-1, MPNST-1, Leiomyosarcoma VS MPNST-1, Leiomyosarcoma VS synovial sarcoma-1, highgrade myxofibrosarcoma-1 with 1 metastatic (Synovial sarcoma) and 2 recurrent lesion (MPNST, Myxofibrosarcoma). Myxofibrosarcomas are considered to be tumors showing intermediate grade of differentiation but due to presence of numerous mitoses and necrosis, it has been graded as grade III using three-tier system. On cytology also, it was grade III and called as spindle cell sarcoma with myxoid change
There were 13 recurrent and metastatic cases. Histopathology was available in 10 cases which included three cases of grade III, five cases of grade II, two cases of grade I on histology. Grade III cases on histology included Angiosarcoma, MPNST, Synovial sarcoma. All these cases were grade III on cytology also. Grade II cases on histology included Synovial sarcoma (two), MPNST (one), Fibrosarcoma (two). All these cases were grade II on cytology also.
There were two recurrent Grade I lesions on histology which were called as grade II on cytology. They included Synovial sarcoma (one), Myxofibrosarcoma (one). Final histology grading was done on cell block (1- Synovial sarcoma), resection (Myxofibrosarcoma). This can be attributed to cytologic over interpretation on recurrent lesions as it is generally thought that recurrent lesions tend to be more aggressive. However Synovial sarcomas are considered high-grade tumors.
There was an overall 81% cytologic and histologic concordance for grading as compared to Mathur et al14 however low as compared to Weir et al2 and Chauhan et al.
Table 3
| S.No | Name of the study | Cyto-histo concordance for grading |
| 1 | Weir et al | 92% |
| 2 | Mathur et al | 74% |
| 3 | Chauhan et al | 88% |
| 4 | Present study | 81% |
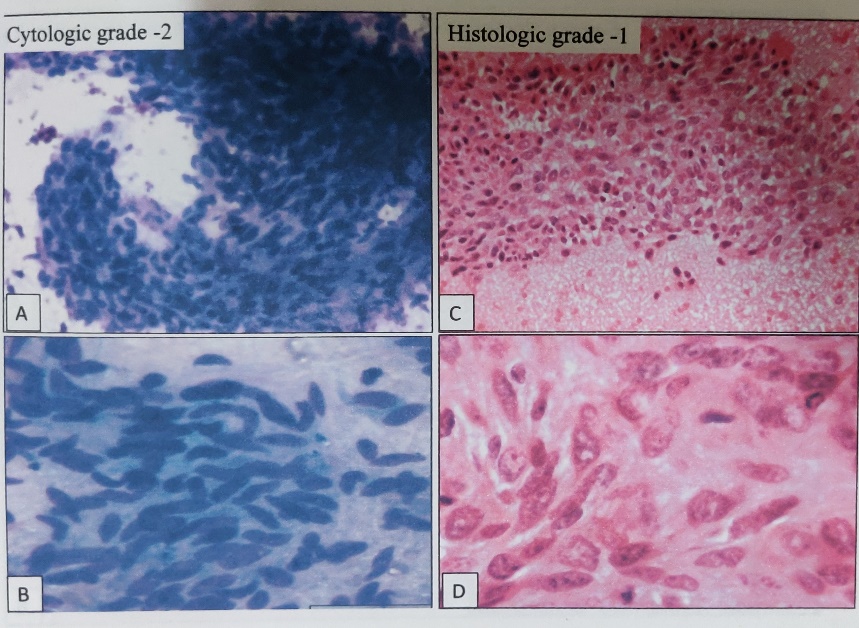
Major discordance (n=3): All the three Grade I lesions on histology were called as Grade II on cytology. Final histology sample was in the form of cell block (one) [Figure 4], biopsy (one), resection (one). Lesions are Synovial sarcoma (one), Recurrent myxofibrosarcoma(one), Spindle cell tumor (one). Discordance could be attributed to limited sample size in two cases. Coinder et al17 has pointed out that biopsy and cell blocks can be misgraded due to sampling error specially since the necrosis and mitosis cannot be correctly assessed. These perhaps are the reason for discordance in two of our cases A case of synovial sarcoma was graded as 1 in cell block. However, they are considered high grade tumors. Discordance in third case could be due to cytological over interpretation of nuclear atypia and overlap (Figure 4)
Figure 3
Major discordance: (A, B): (Giemsa 100x, 200x)- Grade II on cytology; (C, D): (H&E 100x,200x)- corresponding histology on cell block showing grade I
Minor Discordance was seen in three cases. Two Grade III on cytology were Grade II on histology and one Grade II was Grade III. Final histology Sample was in the form of cell block in one case. The lesions included Synovial sarcoma-1; Leiomyosarcoma vs. MPNST-1; Leiomyosarcoma vs Synovial sarcoma-1.
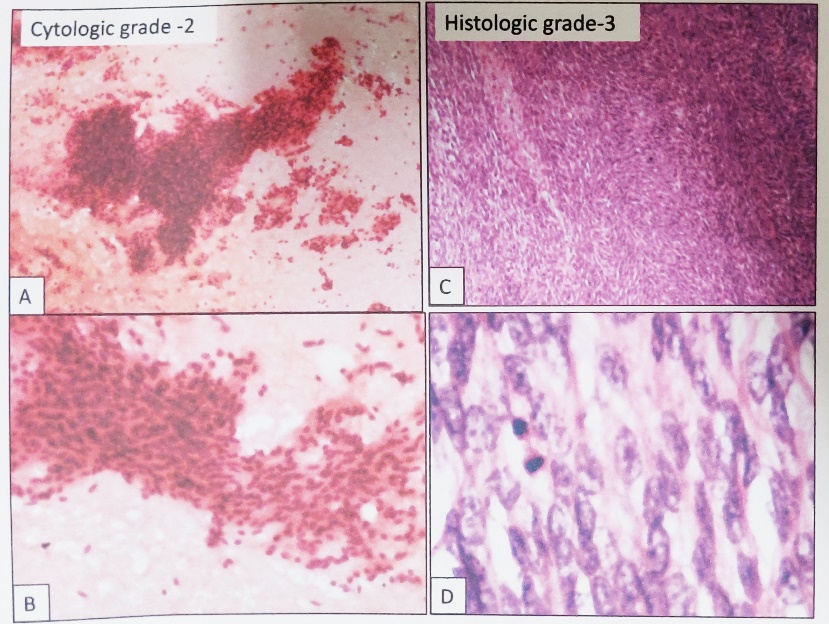
Minor discordance of Grade II lesion (on cytology grade II which turned out be grade III on histology) was seen in one case (Figure 4). In this case, FNAC was done outside and smears were reviewed at our department. Final grading was done on review slides which were two in number. This can be attributed to sampling error or limited material on cytology for grading.
Figure 4
Minor discordance: (A, B): (Pap 40x, 100x)- Grade II on cytology; (C, D): (H&E 100x,200x)- corresponding histology on resection showing Grade III
Minor discordance of Grade III lesions (called as Grade III on cytology but final histology Grade was II) was seen in two cases. In the first case, the final histology was in the form of cell block (limited sample size). In the 2nd case, cytology material was from metastatic site on which grading was done. Final histology grading was done on resected specimen in this case. FNAC grading was difficult due to sarcoma cells showing spindle and epitheliod features, which may have caused overcalling of nuclear atypia and therefore the grade. However, the possibility of higher grade at the metastatic site could not be excluded either.
The present study does not address the sensitivity or specificity of FNAC or its usefulness for distinguishing benign from malignant lesions.
To summarise, total of 46 cases of spindle cell sarcomas were diagnosed on FNAC during the study period. Sub-typing was possible for synovial sarcomas. Histopathology was available in 34 cases. Cytologic-histologic correlation of grading was done. There is a concordance rate of 81.8%.
Major discordance was seen in three cases: Reasons include limited sample size on histopathology (cell block, biopsy) in two cases and due to cytologic over interpretation of nuclear atypia and overlap in third case.
Minor discordance was seen in three cases: Reasons include over grading on cytology in two cases, due to sampling error in third case.
To conclude, FNAC is a valuable tool in pre-operative diagnosis of soft tissue lesions due to low cost, easy procedure, lack of complications and the rapidity with which a diagnosis can be given.
Primary diagnosis of sarcoma is possible on FNAC with good clinical and imageological correlation along with the use of ancillary techniques like Immunocytochemistry
Sub-typing is challenging for spindle cell sarcomas due to complex heterogeneity and morphological overlap. Subtyping is possible for Synovial sarcomas.
There is an overall 81.8% concordance on grading. Though useful, Cytologic grading cannot be used as a single tool for prognostication.
Histologic criteria for grading also has drawbacks and need to be redefined so that it can be applied to micro-biopsy. There is a need to modify the histologic criteria of grading so that more accurate and precise Cytologic grading can be possible.